Volume 1, Chapter 18 - Human Health
Summary
This chapter assesses the impact of the A9 Dualling Programme: Pass of Birnam to Tay Crossing on human health with particular focus on the communities of Dunkeld, Little Dunkeld, Birnam and Inver.
The assessment has followed Design Manual for Roads and Bridges LA 112 ‘Population and human health’ guidance, supported by assessment criteria from the Institute of Environmental Management and Assessment. The assessment has drawn on information from other Environmental Impact Assessment topic chapters as well as from community engagement and desk studies. The following health determinants have been assessed:
- community, recreational and education facilities and severance/separation of communities from such facilities;
- landscape amenity and green/open space and severance/separation of communities from such facilities;
- healthcare facilities and severance/separation of communities from such facilities;
- community identity, culture, resilience and influence;
- spatial characteristics of the transport network and usage, including the surrounding road network, Public Rights of Way (including bridleways), cycle ways, non-designated public routes and public transport routes;
- air quality;
- noise and the ambient noise environment;
- sources and pathways of potential pollution;
- road safety; and
- flood risk.
The significant negative health effects identified relate to construction impacts on noise and the ambient noise, and road safety for vulnerable groups. Disruption of the transport network could have a wider impact on people in the area through safety concerns for commuting or recreational walkers, wheelers, cyclists or horse riders (WCH). Temporary diversions of pedestrians and cyclists may increase the likelihood of collisions with traffic if not appropriately managed and the presence of construction works could also result in a reduction in perceived safety. This localised disruption to pedestrian and cycle routes, as well as to traffic on the A9 and connected road network, would potentially affect access to community, recreational and education facilities, green/open space and healthcare facilities. These are interrelated impacts on transport and access to community and recreational resources. Construction noise and traffic would also affect local amenity. In terms of population health, construction noise impacts could result in a temporary change in quality-of-life with many of those exposed being in residential properties or those wanting to enjoy the outdoor natural heritage of the area. Vulnerable groups may include those with autism spectrum disorder or who have mental health conditions, or shift workers trying to sleep during the day, who are more likely to have a high sensitivity towards noise. The identified pathways to health outcomes from these impacts include reduced physical activity, social interaction and loss of amenity, which may have a negative impact on physical and/or mental health and social wellbeing. While the general population is relatively healthy and likely to be able to adapt, vulnerable groups may have less capacity to adapt to the construction phase impacts and are more likely to suffer adverse health outcomes in the short-term. Mitigation for impacts on traffic, accessibility, land use, noise and air quality are identified in other relevant chapters, while the standard mitigation in the form of the appointment of a Community Liaison Officer, a liaison team and dedicated helpline, is considered particularly important in supporting the affected communities.
For the operation phase, vulnerable groups have the potential to significantly benefit from accessibility and safety improvements to the A9 road and some local routes for WCH. These improvements are expected to reduce physical barriers as well as safety concerns, which may help vulnerable groups in particular to better access community and health facilities, and areas of recreational value. This should support better health and wellbeing. Potential negative effects of the operation stage relate to risks of windblown soil dust and fibres identified in the geology and soils assessment (Chapter 13) and an increase in flood risk for a small number of properties (Chapter 19) which would have potential consequential effects on the health and wellbeing of those affected. However, with proposed mitigation in place these impacts would be reduced to not significant, removing the likelihood of significant health effects.
While there would be significant negative effects on health during the construction stage in the short term for those most affected by noise and disruption, during operation, the significant effects are expected to be positive, relating to improved safety and accessibility.
Introduction
Overview
- This chapter presents the Design Manual for Roads and Bridges (DMRB) Stage 3 Environmental Impact Assessment (EIA) for the A9 Dualling Programme: Pass of Birnam to Tay Crossing (hereafter referred to as the proposed scheme) in relation to impacts on human health.
- The World Health Organization (WHO) defines human health as ‘a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity’ (WHO, 1948). Therefore, this assessment addresses both physical and mental health.
- The assessment considers the potential impacts of the proposed scheme on health determinants, which are the range of personal, social, economic and environmental factors that determine the health status of individuals or populations. The assessment focuses on effects on population health which is defined as the health outcomes of a population, including the distribution of such outcomes within the population (Kindig and Stoddart, 2003), rather than the health of individuals (which is a clinical matter).
- This chapter has drawn on the assessments of residual effects from other EIA topics. Output from the following EIA topics has been considered in the human health assessment:
- Chapter 8 (Air Quality).
- Chapter 10 (Landscape).
- Chapter 11 (Visual).
- Chapter 13 (Geology and Soils).
- Chapter 15 (Noise and Vibration).
- Chapter 16 (Population - Land Use).
- Chapter 17 (Population - Accessibility).
- Chapter 19 (Road Drainage and the Water Environment).
- Chapter 12 (Biodiversity) and Chapter 14 (Material Assets and Waste) are not referenced within this assessment as it is considered that impacts arising from these topics would not have likely significant effects on human health. Chapter 20 (Climate) is also not referenced as localised impacts that could potentially occur as a result of climate change (i.e. flooding) are captured within Chapter 19 (Road Drainage and the Water Environment).
- This chapter does not seek to repeat text or replicate data from other EIAR chapters but instead uses the information to conclude how changes to health determinants could lead to different health outcomes for communities as a result of the proposed scheme.
Legislative and Policy Background
- This section provides an overview of the relevant national, regional and local planning policies for human health and wellbeing.
- The inclusion of the human health topic as part of EIA is a requirement of the EIA Directive (85/337/EEC) (hereafter referred to as the EIA Directive) and The Roads (Scotland) Act 1984 Environmental Impact Assessment) Regulations 2017 (hereafter referred to as the 2017 Roads EIA Regulations). Improving public health and wellbeing in Scotland is the focus of a number of government strategies. In 2018, a Review of Public Health Priorities for Scotland (Scottish Government, 2018) was published which stated that Scottish people have a lower life expectancy than their counterparts in Western Europe. The report set out four priorities, including reducing health inequalities as a primary objective, and also recognising the importance of initiatives such as community gardens and preserving and enhancing walking/cycling routes and greenspace for encouraging physical activity.
Scotland’s National Performance Framework
- In June 2018, the Scottish Parliament introduced the National Performance Framework (NPF), which sets out the vision for national wellbeing in Scotland across a range of economic, social and environmental factors. The NPF sets out 11 ‘national outcomes’. The NPF national indicators have been considered in this assessment as policy priorities of relevance to health and wellbeing.
Transport Scotland’s National Transport Strategy 2
- Scotland’s second National Transport Strategy (NTS2) was published in 2020 and sets out the vision for the country’s transport system, underpinned by four priorities each with three associated outcomes, to be at the heart of decision-making. One of the priorities and associated outcomes is specifically related to health and wellbeing, as follows:
- ‘Improves our health and wellbeing
- Will be safe and secure for all
- Will enable us to make healthy travel choices
- Will help make our communities great places to live.’ (Transport Scotland, 2020)
- NTS2 identifies safety as a priority for the transport system as road incidents can have a significant negative effect on society, with those living in deprived areas being worst affected. Rural areas are also highlighted as a key area for improving safety due to the challenges associated with the more poorly maintained footpath networks and roads.
- NTS2 sets out that active travel is one of the most effective ways to secure the recommended 30 minutes of moderate activity per day to reduce obesity and other health issue related to inactivity. NTS2 highlights the importance of children learning healthy behaviours such as walking or cycling when they are at a young age.
Summary of Sustainable Development and Planning Policies of Relevance to Human Health
- Table 18.1 sets out the key planning policies of relevance to human health and the level at which they are adopted. Section 18.7 provides a summary of the assessment of policy compliance for this chapter and an assessment of the compliance of the proposed scheme against planning policies and plans is also reported in Appendix A3.1 (Plans and Policies).
Table 18.1: Overview of Key Planning Policy Relevant to Human Health
|
Policy |
Description |
Key Points |
|
International |
||
|
United Nations Sustainable Development Goals (United Nations, 2015) |
The SDGs comprise 17 Goals to Transform Our World. They are a call for action by all countries to promote prosperity while protecting the planet. |
‘Goal 3: Ensure Healthy Lives and Promote Well-being for All Ages’ focuses on eradicating diseases and addressing many different and emerging health issues. Health is essential for sustainable development and most of the other goals have an interrelationship with determinants of health. As a result, arguably all of the SDGs can be associated with health in some form. However, some other goals of note are SDG 5 (gender equality), 8 (decent work and economic growth), 10 (reduced inequalities) and 11 (sustainable cities and communities). |
|
National |
||
|
Scotland’s Fourth National Planning Framework (NPF4) (Scottish Government, 2023a) |
NPF4 supports the SDGs and national outcomes and sets out the National Spatial Strategy to improve people’s lives by making sustainable, liveable and productive places. |
In relation to health, the policies outlined in the strategy include:
|
|
Scotland’s National Performance Framework (Scottish Government, 2019) |
NPF sets out ‘national outcomes’ which align with the SDGs and aims to increase the wellbeing of people living in Scotland, amongst other aims. |
The ‘national outcomes’ describe the kind of Scotland it aims to create. In relation to health, the outcomes are as follows:
|
|
Public Health Priorities for Scotland (Scottish Government, 2018) |
This plan sets the national public health priorities for Scotland. |
Priorities relevant for the design of the Scheme include: Priority 1: A Scotland where we live in vibrant, healthy and safe places and communities. Priority 3: A Scotland where we have good mental wellbeing; Priority 5: A Scotland where we have a sustainable, inclusive economy with equality of outcomes for all; Priority 6: A Scotland where we eat well, have a healthy weight and are physically active. This priority promotes physical activity through nature-based initiatives and the maintenance of active travel network. These priorities reflect a holistic approach to public health addressing not only healthcare issues but also the wider determinants of health. This assessment considers wider determinants of health. |
|
Mental Health Strategy 2017 – 2027 (Scottish Government, 2017) |
Sets out 40 initial actions to better join up mental health services, refocus them and deliver them when they are needed. |
The Strategy sets out a guiding ambition for mental health ‘…that we must prevent and treat mental health problems with the same commitment, passion and drive as we do with physical health problems. That means working to improve: This strategy has now been replaced by the Mental Health and Wellbeing strategy below, but this strategy is still relevant due to other policy still being based on this older version. For example, this mental health strategy has informed the Perth & Kinross Mental Health and Wellbeing Action Plan outlined below. |
|
Mental Health and Wellbeing Strategy (Scottish Government, 2023b) |
This Strategy lays out the long-term vision and approach to improving the mental health and wellbeing of everyone in Scotland – including consideration of the role of poverty, housing, employment and communities. |
The Strategy takes an outcome focussed approach with three key areas of focus: ‘Promote positive mental health and wellbeing for the whole population, improving understanding and tackling stigma, inequality and discrimination; Prevent mental health issues occurring or escalating and tackle underlying causes, adversities and inequalities wherever possible; and Provide mental health and wellbeing support and care, ensuring people and communities can access the right information, skills, services and opportunities in the right place at the right time, using a person-centred approach.’ There are nine summary outcomes outlined in the Strategy: 1. ‘Improved overall mental wellbeing and reduced inequalities. 2. Improved quality of life for people with mental health conditions, free from stigma and discrimination. 3. Improved knowledge and understanding of mental health and wellbeing and how to access appropriate support. 4. Better equipped communities to support people’s mental health and wellbeing and provide opportunities to connect with others. 5. More effective cross-policy action to address the wide-ranging factors that impact people’s mental health and wellbeing. 6. Increased availability of timely, effective support, care and treatment that promote and support people’s mental health and wellbeing, meeting individual needs. 7. Better informed policy, support, care and treatment, shaped by people with lived experience and practitioners, with a focus on quality and recovery. 8. Better access to and use of evidence and data in policy and practice. 9. A diverse, skilled, supported and sustainable workforce across all sectors.’ |
|
Strategic Transport Projects Review 2 (STPR2) (Transport Scotland, 2022) |
The STPR2 will inform transport investment in Scotland for the next 20 years (2022-2042) by providing evidence-based recommendations on which Scottish Ministers can base future transport investment decisions. |
The outcomes from STPR2 will:
STPR2 makes 45 recommendations that focus investment on sustainable transport options. The following are considered to be of particular benefit to the Tay Cities region:
|
|
Local |
||
|
Perth & Kinross Council Local Development Plan (LDP) (Perth & Kinross Council, 2019) |
Perth & Kinross Council LDP sets out the overall spatial planning policy for the local authority area. |
Policy 54: Health and Safety Consultation Zones ‘In determining planning applications for development within the Pipeline Consultation Zones identified on the proposals, inset maps and Appendix 3, the Council will seek and take full account of the advice from the Health and Safety Executive and the facility’s operators and owners. The Council will also seek the advice of the Health and Safety Executive and the facility’s operators and owners on the suitability of any proposals for a new notifiable installation within the Plan area or any proposal within the consultation zone of any other notifiable installation.’ (p.91, Perth & Kinross Council, 2019) Policy 52: New Development and Flooding ‘Within the parameters as defined by this policy the Council supports the delivery of the actions and objectives to avoid an overall increase, reduce overall, and manage flood risk as set out within the relevant SEPA Flood Risk Management Strategies and the Local Flood Risk Management Plans. There will be a general presumption against proposals for built development or land raising on a functional flood plain and in areas where there is a medium to high risk of flooding from any source, or where the proposal would increase the probability of flooding elsewhere. In addition, built development should avoid areas at significant risk from landslip, coastal erosion, wave overtopping and storm surges.’ (p.86, Perth & Kinross Council, 2019) Policy 56: Noise Pollution ‘There will be a presumption against the siting of development proposals which will generate high levels of noise in the locality of existing or proposed noise sensitive land uses and similarly against the locating of noise sensitive uses near to sources of noise generation. In exceptional circumstances, where it is not feasible or is undesirable to separate noisy land uses from noise sensitive uses, or to mitigate the adverse effects of the noise through the negotiation of design solutions, the Council may use conditions attached to the granting of planning consent, or if necessary planning agreements, in order to control noise levels. A Noise Impact Assessment will be required for those development proposals where it is anticipated that a noise problem is likely to occur.’ (p.91, Perth & Kinross Council, 2019) Policy 57: Air Quality ‘The Council has a responsibility to improve air quality. The LDP does this by seeking to prevent the creation of new pollution hotspots, and to prevent introduction of new human exposure where there could be existing poor air quality. The LDP extends support to low emission technologies for both transport and energy production. As well as aspiring to improve air quality, the policy also aspires to eliminate the gradual worsening in air quality that is caused by the cumulative impact of many small developments. Within or adjacent to designated Air Quality Management Areas, where pollutant concentration are in excess of the national air quality objectives and may pose a risk to human health, development proposals that would adversely affect air quality may not be permitted. There is a presumption against locating development catering for sensitive receptors in areas where they may be exposed to elevated pollution levels. Any proposed development that could have a detrimental effect on air quality, through exacerbation of existing air quality issues or introduction of new sources of pollution (including dust and/or odour), must provide appropriate mitigation measures. The LDP expects that some type of mitigation of air quality impacts will be required for all but the smallest developments. Best practice design measures should therefore be considered early in the design and placemaking process. Proposals and mitigation measures must not conflict with the actions proposed in Air Quality Action Plans.’ (p.92, Perth & Kinross Council, 2019) Policy 58A: Contaminated Land ‘The Council’s first priority will be to prevent the creation of new contamination. Consideration will be given to proposals for the development of contaminated land, as defined under Part IIA, Section 78A(2) of the Environmental Protection Act 1990, where it can be demonstrated to the satisfaction of the Council that appropriate remediation measures can be incorporated in order to ensure the site/land is suitable for the proposed use and in order to ensure that contamination does not adversely affect the integrity of a European designated site(s). Informal pre-application discussions should take place at the earliest opportunity between the Council, the developer and any other interested parties in order to help identify the nature, extent and type(s) of contamination on the site (including any source, pathways, receptor links) and the most appropriate means of remediation. The Council may attach conditions to the granting of planning consent to ensure that these remediation measures have been completed prior to the commencement of any works on site and/or the occupation of any new units. The Council will adopt the ‘suitable for use’ approach as advocated by Scottish Government Statutory Guidance when dealing with proposals for the development of contaminated land.’ (p.95, Perth & Kinross Council, 2019) |
|
Mental Health and Wellbeing Action Plan (Perth & Kinross Council, 2018) |
The Plan had been developed to direct services towards new ways of working to ensure people get the support they need at the right time and is strategically aligned to National Health and Wellbeing Outcomes. |
The Plan sets out local mental health and wellbeing outcomes, which are guided by the broader national outcomes. Examples of these local outcomes are as follows (the list is not exhaustive):
|
|
A9 Dualling Programme Strategic Environmental Assessment (SEA) (Transport Scotland, 2013) |
The SEA aimed to integrate environmental considerations into the very early stages of programme development for the A9 Dualling Programme. |
The SEA highlighted the following as considerations for population and human health. The A9 Dualling Programme was considered to be an opportunity to improve road safety, reduce accident severity and improve connectivity between Inverness, Perth, local communities and the central belt. The SEA also flagged access to/from the route, particularly regarding walkers, cyclists and horse riders, the Cairngorms National Park and other recreational facilities, as key challenges. |
Approach and Methods
- This section explains the approach used to establish the baseline conditions and assess the potential changes to health outcomes and includes a summary of the relevant guidance used in the human health assessment.
Overall Approach
- The assessment follows DMRB LA 112 ‘Population and human health’ guidance of the effects of proposed trunk road schemes on human health (hereafter referred to as DMRB LA 112) (National Highways et al., 2020). The assessment uses the Institute of Environmental Management and Assessment (IEMA) Guide to Determining Significance for Human Health in Environmental Impact Assessment (Pyper et al., 2022a) in the assessment of likely significant effects and considers the health determinants outlined in the IEMA Guide to Effective Scoping of Human Health in EIA (Pyper et al., 2022b). The six stages of the human health assessment which have been developed for this EIA are outlined in Diagram 18.2.
Background
- During DMRB Stage 2, in response to community consultation, a Wellbeing Assessment was undertaken using a bespoke approach and methods. The community objectives (as shown in Table 18.2) were mapped against wellbeing indicators drawn from Scotland’s National Performance Framework (refer to Table 18.1) and assessed against the output from relevant chapters of the DMRB Stage 2 report to reach a conclusion as to whether the route options would contribute to the realisation of the community objectives. The assessment also aimed to identify which of the route options would have the most impact on wellbeing outcomes.
- The process of developing the community objectives allowed the key concerns of the communities to be considered during the optioneering stage. The route options that performed more favourably against the community objectives were assessed as having the potential for positive health and wellbeing outcomes. As a result of the development of community objectives, the scope of the human health assessment was extended. The DMRB Stage 2 Human Health assessment applied a robust approach at the time of publication, both meeting and going beyond the minimum requirements of the DMRB LA 112 standard through the additional consideration of cultural heritage and associated wellbeing impacts.
The IEMA Guide to Effective Scoping of Human Health in EIA (Pyper et al., 2022b) has been published since the preparation of the DMRB Stage 2 Human Health assessment. The consideration of cultural heritage and associated wellbeing impacts as identified in the DMRB Stage 2 Human Health assessment aligns closely with the description of the wider determinant of ‘community identity, culture, resilience and influence’ from the more recent IEMA scoping guidance. Therefore, for this Stage 3 human health assessment the terminology from the IEMA guide has been used (‘community identity, culture, resilience and influence’) to describe the additional health determinant for consistency with this newer guidance, which is increasingly being regarded as the standard approach for human health assessment in EIA.
Diagram 18.2: Methodology for A9 DMRB Stage 3 Human Health Assessment
Characterise population
- Identify population groups potentially exposed to impacts of proposed scheme (i.e. neighbours, recreational groups, business owners).
- Develop a health profile of the population to take account of health and socio-economic characteristics.
- Identity vulnerable groups
within the population which may have increased susceptibility to certain health impacts.
Identify baseline health determinants
- Obtain data on quality of biophysical, social and economic environmental conditions that reflect the health determinants listed in DMRB LA 112.
- Identify assets important to community health and wellbeing. Use the community objectives to ensure this is done through a local lens.
Identify and assess potential impacts on determinants
- Identify how the proposed scheme could impact on the baseline health determinants.
- Estimate the scale (magnitude) of impact from the proposed scheme and the characteristics of the impact (i.e. whether it is permanent or temporary, widespread or localised etc.)
Identify potential health effects
- Identify associated health outcomes, based on literature review of health research.
Estimate what proportion of the community is likely to be affected. - Consider potential differences in outcomes between vulnerable groups and general population.
- Consider whether health inequalities may be widened or narrowed by impacts.
Identify mitigation and enhancement measures
- Identify measures which could reduce negative health impacts, improve health outcomes and reduce health inequalities.
Conclude assessment
- Describe key residual health outcomes associated with impacts of the proposed scheme.
- Conclude as to whether the outcomes would be positive or negative and determine the likely significance level.
- Conclude as to whether health inequalities are expected to be widened or narrowed by the impacts.
Table 18.2: Birnam to Ballinluig A9 Community Group Community Objectives
|
Community Objective Ref. |
Community Objective Description |
|
1
|
Reduce current levels of noise and pollution in the villages of Dunkeld, Birnam and Inver to protect human health and wellbeing of residents and visitors and to enable them to peacefully enjoy their properties and amenity spaces. |
|
2
|
Protect and enhance the scenic beauty and natural heritage of the area and its distinctive character and quality. |
|
3
|
Provide better, safer access on and off the A9 from both sides of the road while ensuring easy, safe movement of vehicular traffic and WCH through the villages, helping to reduce stress and anxiety and support the local community. (Non Motorised Users (NMUs) in the DMRB Stage 2 assessment are referred to as Walkers, Cyclists and Horse-riders (WCH) in accordance with DMRB LA 112) |
|
4
|
Promote long-term and sustainable economic growth within Dunkeld and Birnam and the surrounding communities. |
|
5
|
Examine and identify opportunities to enhance the levels of cycling and walking for transport and leisure, including the improvement of existing footpaths and cycle ways, to promote positive mental health and wellbeing. |
|
6
|
Ensure that all local bus, intercity bus services and train services are maintained and improved. |
|
7
|
Preserve and enhance the integrity of the unique and rich historical and cultural features of the Dunkeld, Birnam and Inver communities, thereby supporting wellbeing and the local economy. |
Community Participation and Engagement
- While this DMRB Stage 3 human health assessment has been prepared to meet the requirements of the EIA Directive, it also adopts some of the International Association of Impact Assessment’s (IAIA) best practice principles for Health Impact Assessment (Winkler et al., 2021) through the use of community participation and engagement to inform the assessment and seek opportunities for health improvement.
- At an early stage of the A9 Co-Creative Process, the Birnam to Ballinluig A9 Community Group generated a set of community objectives (as shown in Table 18.2). The A9 Co-Creative Process has influenced the human health assessment and design of the proposed scheme through early engagement. This early engagement has also helped to inform the scope and identified matters that are of importance to the community. This has allowed the community to have more control through inclusion and participation in the process. The IAIA also states that, as one of the guiding principles of HIA:
‘HIA should involve and engage stakeholders so that people potentially affected by the development initiative have an opportunity to express their hopes and concerns regarding health and can influence the formulation of public health actions’ (Winkler et al., 2021).
- This principle has been considered, and will continue to be, through the community objectives. These community objectives have identified the health priorities for the area regarding what is important to the communities in relation to their health and wellbeing.
- The community objectives identified at DMRB Stage 2 capture local community participation in the assessment process. The human health assessment has considered the community objectives as well as public consultation undertaken for DMRB Stage 3 during summer 2024 (Section 7.4, Chapter 7: Consultation and Scoping), to help inform the understanding of community priorities and views, as well as informing the judgement of significance in line with the IEMA Guide to: Determining Significance of Human Health In Environmental Impact Assessment (Pyper et al., 2022a). To date, consultation undertaken during DMRB Stage 3 has included community engagement events in August 2024, which provided the community the opportunity to feedback any further suggestions on incorporating the objectives within the design and assessment work. Engagement with three local schools was also undertaken during this time to ensure that children’s concerns are also taken into account. Relevant information gathered from this engagement has been used to inform the human health assessment reported in this chapter, and is referenced where relevant in Section 18.3 Baseline Conditions and Section 18.4 Potential Impacts and Effects.
Study Areas
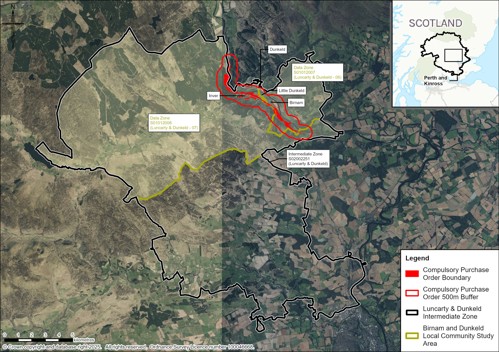
- The main human health study area is comprised of the 2011 data zones of S01012007 and S01012008, with a particular focus on the following communities within the study area which coincide with a 500m buffer of the proposed scheme: Birnam, Little Dunkeld, Dunkeld and Inver, which reflect the study areas applied in Chapter 16 (Population - Land Use) and Chapter 17 (Population - Accessibility). It is referred to in this chapter as the ‘Birnam and Dunkeld Community Study Area’. Data Zones are composed of Census Output Areas large enough to present statistics accurately without fear of disclosure and small enough that they can used to represent communities. The 2011 data zones were selected to ensure consistency and comparability of data. For example, the Scottish Index of Multiple Deprivation uses the 2011 Data Zones.
- The location of the communities are shown on Image 18.1. It was considered that there is limited potential for significant human health impacts outside the 500m population study area. However, it is recognised that there are smaller settlements – such as Dalmarnock and Dalguise – and residences in the wider area from which people may access community, education, and healthcare facilities within Dunkeld, Little Dunkeld, Birnam and Inver. The populations within these settlements and residences are considered in the assessment where relevant. For some health data, it was necessary to apply the Intermediate Zone as data were not available for areas as small as the data zones. Where the Intermediate Zone has been applied it is referred to in this chapter as the ‘Luncarty and Dunkeld Community Study Area’. Some health data are only available at regional level, in which case the Perth & Kinross Council area has been used as the study area. The study areas are indicated on Image 18.2.
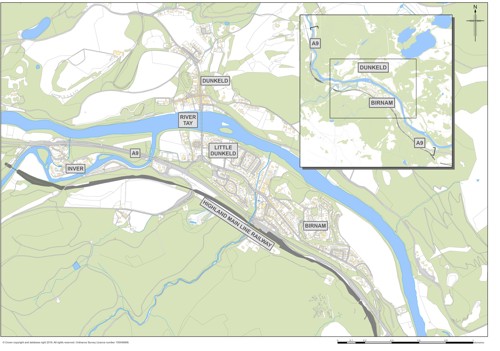
Table 18.3 describes the location of the communities within 500m of the proposed scheme. The communities of Birnam, Little Dunkeld and Dunkeld each straddle two data zones, the location of the data zone relative to the community is included in the data zone column in Table 18.3.
Table 18.3: Human Health Assessment Study Area – Key Communities
|
Community |
Data Zone(s) |
Description |
|
Birnam |
S01012007 (north) S01012008 (south) |
Birnam straddles two data zones, the location of the data zone relative to the community is included in the data zone column. Community located between ch2500 and ch3450 of the proposed scheme that could be subject to potential impacts on human health. |
|
Little Dunkeld |
S01012007 (north) S01012008 (south) |
Community located between ch3450 and ch4300 of the proposed scheme that could be subject to potential impacts on human health. |
|
Dunkeld |
S01012007 (east) S01012008 (west) |
Community located approximately 500m north of the proposed scheme that could be subject to potential impacts on human health. |
|
Inver |
S01012008 |
Community located between ch4700 and ch5100 of the proposed scheme that could be subject to potential impacts on human health. |
Additionally, the EIA topics pertinent to the human health assessment each have their own study areas. These are outlined in Table 18.4. Data gathered on the study areas from these topics have been applied to the communities identified for the human health assessment where appropriate.
Table 18.4: Study Areas Defined in Technical Chapters of the EIAR
|
Chapter |
Study Area |
|
Chapter 8 (Air Quality) |
Sensitive receptors at risk of being affected by dust, including residential and other sensitive properties as well as designated sites were identified within 200m of the affected road network using Ordnance Survey (OS) Address Base Plus and Scottish Natural Heritage (SNH) datasets. The extent of road links considered for the assessment of vehicle emissions from construction traffic included all roads within 500m (north and south) of the proposed scheme mainline, scoped against the DMRB LA 105 (National Highways et al., 2024) screening criteria. |
|
Chapter 9 (Cultural Heritage) |
A study area comprising the Compulsory Purchase Order Area plus an area extending 200m in all directions from it is defined. Consultation with the noise specialists identified that the extent of the study area was sufficient to identify and assess potential noise effects on the setting of cultural heritage resources. The Zone of Visual Influence (or Zone of Theoretical Visibility) was used to identify cultural heritage resources outside the study area the settings of which could be affected by the proposed scheme. Where the potential for an effect on the setting of a cultural heritage resource was identified, these cultural heritage resources were included in the cultural heritage baseline. |
|
Chapter 10 (Landscape) |
A study area extending to 5km from the proposed scheme has been adopted for the landscape assessment. Within this 5km study area, Zones of Theoretical Visibility (ZTVs) have been prepared for the existing A9 and the proposed scheme. |
|
Chapter 11 (Visual) |
A study area extending to 5km from the proposed scheme has been adopted for the visual assessment. Within this 5km study area, Zones of Theoretical Visibility (ZTVs) have been prepared for the existing A9 and the proposed scheme. |
|
Chapter 13 (Geology and Soils) |
The assessment covers a study area extending to a corridor of 250m from the compulsory purchase order boundary of the proposed scheme. For Groundwater Dependant Terrestrial Ecosystems (GWDTE), as agreed with the Scottish Environment Protection Agency (SEPA), a study area extending 100m from the existing A9 was used, and extended where required, for the purpose of dewatering impact assessments. The study area for groundwater abstractions is within 1.2km of the compulsory purchase order boundary. Typically, the minimum study area to be applied for groundwater abstraction licensing is 850 m under The Water Environment (Controlled Activities) (Scotland) Regulations 2011 and based on ‘Regulatory Method (WAT-RM-11) Abstraction from Groundwater V6’ (SEPA, 2017). However, following consultation with SEPA it was agreed the study area would be expanded to 1.2 km for abstractions (see Chapter 13 for further information). |
|
Chapter 15 (Noise and Vibration) |
A construction noise study area of 300m around the proposed scheme footprint boundary has been defined. A construction vibration study area of 100m around the proposed scheme footprint boundary has been defined. The operational noise assessment approach and methods includes an area within 600m of new road links or road links physically changed or bypassed by the project and an area within 50m of other road links with potential to experience a short-term basic noise level change of more than 1.0dB(A) as a result of the project. Operational vibration was scoped out of the assessment. |
|
Chapter 16 (Population - Land use) |
In accordance with DMRB LA 112, the initial study area for this assessment is based on the construction footprint/boundary (including temporary land-take) plus a 500m area. The guidance also states that where appropriate, the study area may be reduced or extended to support the impact assessment. In considering severance, cognisance is taken of any change in traffic volumes outwith 500m as a result of the proposed scheme. |
|
Chapter 17 (Population - Accessibility) |
The study area for the assessment of impacts on WCHs includes paths within 500m of the proposed scheme. However, the assessment was also informed by consideration of the wider area, which is particularly important in identifying potential limitations to accessing outdoor areas. The study area for the assessment of changes to views from the road was defined as the route of the existing A9 and the proposed scheme. As the proposed scheme is a dualling of the existing road, a direct comparison between the existing A9 and the proposed scheme could be made. |
|
Chapter 19 (Road Drainage and the Water Environment) |
The baseline study area for this assessment extends 500m from the footprint of the proposed scheme and includes identified water features (‘WFs’: including major to minor watercourses, drainage ditches and palaeo-channels), existing watercourse crossing points and flood inundation extents. Where appropriate, the potential for flood risk impacts associated with the proposed scheme beyond the 500m study area are considered within the assessment. |
Data Collection
- The baseline for the human health assessment has been developed through the following approaches:
- Data collection – using sources such as the Office of National Statistics (ONS), Scottish Index of Multiple Deprivation (SIMD), National Record of Scotland Monthly Data on Births and Deaths Registered in Scotland, 2022 Scottish Census data, National Records of Scotland, Information Services Division (IDS) Scotland website, Local Development Plans and Policy Documents, and others which are referenced where relevant.
- Spatial data mapping – using aerial photography and Ordnance Survey (OS) maps, Jacobs’ Geographical Information System (GIS) database, in addition to the above data sources.
- Consultation – with statutory and non-statutory consultees, as appropriate.
- The human health assessment presented in this chapter has drawn on data used in the DMRB Stage 2 Wellbeing Assessment which has been updated as appropriate to inform the baseline.
Consultation
- During DMRB Stage 3, consultation was undertaken with Perth & Kinross Council, the National Health Service (NHS) Scotland, Emergency Services, as well as continued consultation with the Birnam to Ballinluig A9 Community Group. The assessment has also drawn on feedback from the following consultation events:
- In-person public exhibition January 2024 presented the Preferred Route Option at Birnam Arts & Conference Centre.
- Public exhibitions August 2024, to allow members of the public to see and comment on the development of the proposed scheme design since the Preferred Route was announced.
- September 2024 that was targeted at children and young people from Royal School of Dunkeld, Pitlochry High School and Breadalbane Academy.
- Further details on consultation and scoping are provided in Chapter 7 (Consultation and Scoping). No specific responses regarding the human health assessment scope were received.
Characterising the Population
- In accordance with DMRB LA 112 (National Highways et al. 2020, p.20) a health profile for each of the communities in the study has been established through consideration of the following data where available:
- percentage of community with increased susceptibility to health issues (vulnerable members, e.g. under 16 and over 65);
- percentage of community with pre-existing health issues (e.g. respiratory disease/chronic obstructive pulmonary disease (COPD));
- deaths from respiratory diseases;
- percentage of community with long term illness or disability;
- general health;
- life expectancy; and
- income deprivation.
- Some further health data have also been on mental health indicators to reflect that health includes mental as well as physical wellbeing.
Identifying the Baseline Health Determinants
- As outlined in paragraph 18.1.3, health determinants are the range of personal, social, economic and environmental factors which can influence the health status of individuals or populations. The health determinants included in the scope of assessment are as set out in DMRB LA 112 with one addition, based on the IEMA Guide to Effective Scoping of Health in EIA (Pyper et al., 2022b). As noted above, the consideration of cultural heritage and associated wellbeing impacts was added to the scope of assessment at DMRB Stage 2 in response to the community objectives, and the DMRB Stage 2 Human Health chapter was completed before the publication of the IEMA Guide to Effective Scoping of Human Health in EIA (Pyper et al., 2022b). Therefore, after consideration of the wider health determinants, the additional cultural heritage and associated wellbeing impacts have been determined to align closely with the description of the wider determinant of ‘community identity, culture, resilience and influence’ from the IEMA scoping guidance and was added to the scope of the DMRB Stage 3 human health assessment.
- The scope of health determinants addressed in the baseline and assessment have been assigned a reference number between 1 and 10 (e.g. HD1) and are as follows:
- HD1: community, recreational and education facilities and severance/separation of communities from such facilities.
- HD2: landscape amenity and green/open space and severance/separation of communities from such facilities.
- HD3: healthcare facilities and severance/separation of communities from such facilities;
- HD4: community identity, culture, resilience and influence;
- HD5: spatial characteristics of the transport network and usage in the area, including the surrounding road network, Public Rights of Way (including bridleways), cycle ways, non-designated public routes and public transport routes;
- HD6: air quality;
- HD7: noise and the ambient noise environment;
- HD8: sources and pathways of potential pollution;
- HD9: safety associated with the existing affected road network; and
- HD10: flood risk.
- Where appropriate, baseline information on health determinants has been obtained with cross-references to other assessments in the EIA, for example, the air quality and noise assessments.
Identifying and Assess Potential Impacts on Determinants
- The first step in the identification of impacts was to understand how the baseline health determinants would be likely to be affected by the proposed scheme. A change to a single health determinant can affect the health status of different individuals or communities depending on their characteristics and sensitivity to change, thereby generating multiple health outcomes. Again, for health determinants covered by other topics of this EIA, reference has been made to the relevant topic chapters to identify the nature and scale of impacts on the health determinants.
- The methodology, as set out in DMRB LA 112 and the IEMA guidance, involved the assessment of changes in health determinants and relating these to potential population health impacts through consideration of the local community health profiles and scientific evidence.
Identifying Potential Health Effects
- In order for there to be a potential likely health effect, a health pathway must be established that ‘shows a plausible theoretical link between source-pathway-receptor; and the occurrence of which is judged as probable’ (IEMA, 2022b). As recommended by IAIA’s Human Health: Ensuring a High Level of Protection (IAIA, 2020), a literature review has been undertaken to determine an association between changes that are likely to occur due to the proposed scheme in relation to the health determinants, and the resulting potential changes to health outcomes. The results of the literature review are provided in paragraphs 18.2.27 – 18.2.61.
- Identification of a health pathway does not mean that there would be a significant impact on human health. Professional judgement has been applied using the IEMA assessment criteria (IEMA, 2022a) to determine the level of significance (See ‘Assessment Reporting and Significance Criteria’ below).
- Evidence derived from a literature review for health outcomes, and the interpretation of this evidence for the health determinants considered within this assessment, are summarised below.
Human Health Evidence Associated with Community, Recreational and Education Facilities (HD1), Landscape Amenity, Green/Open Space (HD2), and Healthcare Facilities and Severance/Separation of Communities from Such Facilities (HD3)
- The DMRB LA 112 defines ‘severance’ as ‘the extent to which members of communities are able (or not able) to move around their community and access services/facilities’. However, within transport and health literature, community severance may be applied to any one of, or a combination of, the following impacts: reduction in pedestrian access due to high traffic flows; barrier effect of physical infrastructure; changes in mobility and accessibility; reductions in social contacts; and psychological separation of neighbourhoods. The various definitions of community severance make comparisons of research difficult (Mindell and Karlsen, 2012). There are various recent studies which provide evidence that traffic speed and volume reduces levels of physical activity, social contacts, children’s play and access to goods and services. Anciaes et al. (2016) identify that:
- high levels and speeds of motorised traffic discourage walking; and
- high levels and speeds of motorised traffic limit social contact between residents living on the opposite sides of roads.
- However, the research into associations between community severance and mental or physical health outcomes is limited. Mindell and Karlsen (2012) undertook a systematic review on community severance and health. They identify that Appleyard and Lintell’s study of San Francisco showed a reduction in social contacts due to increased traffic, and that there is research which shows an inverse association between social contacts and mortality risk. However, they could not identify any studies of mortality or morbidity which have examined reductions in social contacts as a result of new roads, increased traffic volumes or traffic speeds. They conclude that:
‘The chain of inference for the health effects of community severance does not currently extend to direct observation. It seems inherently likely that the effects of community severance do indeed impact on health, with adverse health consequences of reduced social contacts also occurring when this social disruption is due to road traffic. Given the scale of the effect on mortality of high social integration, which is of similar magnitude to stopping smoking (Holt-Lundstad et al., 2010) it is of great public health importance that research is conducted to confirm the postulated links and to establish which are the important components of community severance for health and how they can be ameliorated.’ (Mindell and Karlsen, 2012).
- The ability to access shops, recreational facilities and education helps to support the health and wellbeing of communities. Severance to core/local paths, transport networks, open space and community, recreational, educational and healthcare facilities has the potential to impede access and exacerbate health inequalities. This can result in reduced social cohesion and physical activity and have negative impacts on mental health (Mindell and Karlsen, 2012; Marmot et al., 2020).
- The intrinsic qualities of green and blue spaces have been shown to enhance health and wellbeing through connection with nature and cognitive and psychological restoration, the opportunity to perform physical activity through active travel, and enhance social interaction (Gascon et al., 2015; Bray et al., 2022). Coventry et al. (2021) conducted a systematic review on nature-based outdoor activities for mental health in community-based settings which shows that nature-based interventions can effectively improve mental health and wellbeing and that improvements in mental health might be attributed to nature connectedness, social support, physical activity and purposeful behaviour.
- While the formal healthcare services account for only 20% of population health (the other 80% being related to wider determinants of health such as the health behaviours and social, economic and environmental conditions in which people live) (American Hospital Association, 2020), access to healthcare is nevertheless important for individuals and a fundamental human right. Survival rates from out-of-hospital cardiac arrests (Lyon et al., 2004) and stroke (Simonsen et al., 2014) are strongly influenced by emergency response times. Therefore, any delay to emergency admissions caused by traffic disruption could have a significant impact on health outcomes for some individuals who need emergency care.
Interpretation for Assessment
- Large increases in traffic volume or speed, or creation of physical infrastructure which may act as a barrier to pedestrian movement or use of outdoor space for social interaction, has been considered as negative for health, while large reductions in traffic volume or speed, or removal of physical infrastructure which support improved pedestrian movement or use of outdoor space for social interaction, has been considered as positive for health. Given the lack of research on size of effect, or thresholds at which severance may occur, significant effects on health outcomes are judged likely only if changes would be widespread across the human health study area.
- Disruption of access to healthcare facilities (whether by vehicle or on foot) have been considered negative for health. The significance has been judged in relation to the sensitivity of the population, the nature of the health services (i.e. whether emergency care or not) and the scale of impact on access.
Human Health Evidence Associated with Community Identity, Culture, Resilience and Influence (HD4)
- Communities with high levels of social capital (indicated by sets of shared values in a community, participation and working together) have advantages for the mental health of individuals, and these characteristics have also been seen as indicators of the mental well-being or resilience of a community (Cooke et al., 2011).
- Creative activities improve self-esteem, confidence, motivation, happiness and reduce stress and enhance control. Leisure and physical activity enhance well-being by increasing feelings of competency and relaxation, distracting from difficulties, as well as enhancing social inclusiveness and support (Caldwell, 2005). Research has shown that the use of artistic media in health care and in communities can have a variety of benefits for health outcomes. Participation in arts enhances well-being though direct engagement in art activity, although this facilitates social participation which also enhances well-being (Fancourt and Finn, 2019). A systematic overview conducted by Leigh-Hunt et al. (2017) highlights that there is consistent evidence linking social isolation and loneliness to worse cardiovascular and mental health outcomes.
Interpretation for Assessment
- Based on the evidence, the assessment has considered how the proposed scheme may affect the places and activities that local people associate with a sense of their community identity. These aspects will be considered as important for social wellbeing.
Human Health Evidence Associated with Spatial Characteristics of the Transport Network and Usage (HD5)
- A good transport system is essential for a healthy society. The impact of air pollution on health is well-known, but transport affects the health of people across society in multiple ways. Investing in transport is seen as a way to address widening health inequalities and regional disparities in public health. The quality of the transport infrastructure and the adequacy of transport services directly affect health by, for example, enabling active modes of travel (such as walking and cycling) or reducing road accidents and harmful emissions. Wider, indirect impacts on health include enabling people to get to work, school, hospital and fresh food shops, as well as social events and leisure activities – aspects of life that are important for good physical and mental health (as evidenced above). Transport infrastructure and provision can have direct and indirect effects on mental and physical health by supporting access places of employment and study, community and recreational facilities or public transport access points for pedestrians and cyclists.
- The health benefits of regular physical activity are well researched and widely accepted. For most people, the easiest forms of physical activity are those that can be built into daily life, for example, by using walking or cycling as an alternative to motorised transport for everyday journeys such as commuting to work or school. Active forms of travel, such as walking and cycling, are associated with a range of health benefits, including improved mental health, reduced risk of premature death and prevention of chronic diseases such as coronary heart disease, stroke, type 2 diabetes, osteoporosis, depression, dementia and cancer (British Medical Association, 2012). Research also suggests that countries with the highest levels of active travel generally are amongst those with the lowest obesity rates (Bassett et al., 2008).
Interpretation for Assessment
- For the health assessment, increases in transport choices and opportunities for active travel have been considered positive for health on account of health benefits associated with reliable transport and physical exercise, as well as benefits in terms of reducing pollution and other negative aspects of motor vehicles. However, significant impacts on population health outcomes are only predicted where a substantial modal shift to active modes of travel are anticipated.
Human Health Evidence Associated with Air quality (HD6)
- Poor air quality can result in human health conditions such as respiratory problems, cardiovascular disease and lung cancer (Royal College of Physicians, 2016).
- A systematic review conducted by Chen and Hoek (2020) has considered the health effects of air pollution based on health effects from long-term exposure to Particulate Matter (PM). This review provided clear evidence that both PM5 and PM10 were associated with increased mortality from all-causes (natural-cause mortality or non-accidental mortality from all-causes, except external causes such as accidents, suicide and homicide), cardiovascular disease, respiratory disease and lung cancer. A systematic review conducted by Orellano et al. (2020) also found that an increase in outdoor concentrations of PM10, PM2.5, nitrogen dioxide and ozone increases the risk of all-cause and cause-specific mortality in humans.
- A systematic review conducted by Wang et al. (2021) considered the link between short-term exposure to nitrogen dioxide and mortality and identified evidence of association between short-term exposure to nitrogen dioxide and all-cause, cardiovascular and respiratory mortality.
- Based on the scientific evidence from systematic reviews, the WHO Air Quality Guidelines (2021) provide global guidance on threshold and limits for key air pollutants that pose health risks. These guidelines are much more conservative than the current UK Air Quality Objectives (AQO).
- Direct impacts on air quality have been reported in Chapter 8 (Air Quality). As reported in Chapter 8, human exposure to particulate matter (both in the sort and long term) and nitrogen oxides can have adverse health impacts. There is no proven safe threshold at which human health is not at risk from particulate matter.
Interpretation for Assessment
- There is good evidence that transport related air pollutants such as PM10, PM5 and NO2 are associated with an increased risk of a range of health outcomes, including at levels of pollution substantially below the AQO. However, it should be noted that the evidence from the systematic reviews, which underpin the WHO Air Quality Guidelines, are based on relatively small sample sizes and the WHO Air Quality Guidelines are designed to protect large populations from small increases in disease and mortality. For most individuals, the increase in risk posed by outdoor air pollution is extremely low compared to other risk factors, such as diet, smoking and level of exercise.
- It should also be noted that while road traffic contributes to pollution, it is one contributor among many other sources, and in the case of PM, sources such as residential, commercial and public sector combustion (which would include woodburning stoves, bonfires etc.) provide a greater share of the PM emissions.
- Any increase in exposure to air pollution is negative for population health, while any decrease in exposure to air pollution is positive for population health. However, significant impacts on population health (i.e. where a notable change in the level of health outcomes) are only judged likely where the proposed scheme would cause an exceedance of the AQO or where a substantial change in concentrations of pollutants are anticipated compared to the baseline (Do-Minimum). The assessment has also been informed by Chapter 8 (Air Quality).
Human Health Evidence Associated with Noise and the Ambient Noise Environment (HD7)
- High levels of noise nuisance and vibration cause by traffic and construction activities can cause psychological distress (Clark et al., 2020) and there is evidence to suggest increased noise exposure can increase the risk for Ischemic Heart Disease (IHD) and hypertension (Rompel et al., 2021). There is also increased risk of sleep disturbance, hearing impairment, tinnitus and cognitive impairment, with increasing evidence for other health impacts, such as adverse birth outcomes and mental health problems (WHO, 2024). Noise from road traffic alone is the second most harmful environmental stressor in Europe, behind only air pollution from fine particulate matter (WHO, 2018). The harmful effects of noise arise mainly from the stress reaction it causes in the human body, which can also occur during sleep. The Environmental Noise Guidelines for Europe (WHO, 2018) set out recommendations for road traffic noise and other sources of environmental noise, following a series of systematic reviews of the current evidence on the following critical health outcomes: annoyance, sleep disturbance, cardiovascular disease, and cognitive impairment.
Interpretation for Assessment
- Increases in noise levels are considered negative for health, while decreases are considered positive. It is noted that the WHO has considered the evidence sufficient to support a strong recommendation that road traffic noise should be reduced to below 53 dB Lden. This guideline level is benchmarked at the level where 10% of a population are likely to be ‘highly annoyed’. Noise of this level is relatively widespread in the UK, particularly in urban areas. Annoyance is regarded as a relatively mild health effect, as indicated by the disability weighting applied by the WHO.
- The more serious health outcome for which evidence is of a high quality is IHD. This risk is linked to long-term exposure to higher levels of noise. However, it should be noted that the risk of IHD linked to noise is very small compared to other risk factors. Nevertheless, it is a public health issue of concern due to the widespread exposure of populations to traffic noise.
- The assessment has also been informed by Chapter 15 (Noise and Vibration). Health effects have been judged to be significant if the proposed scheme is expected to effect a large change in the noise environment.
Human Health Evidence Associated with Sources and Pathways of Potential Pollution (HD8)
- Air pollution and noise are the main pollutants associated with road transport, as described above. In the context of a road scheme, key sources of pollution would be fuels, oils, cementitious material and other substances used during construction and operation, and the presence of any historical contamination in the ground at the construction site.
- Pathways to exposure could include emissions to air and spillages to water or soil, and disturbance of historical contaminants in the ground via excavations during construction. People have the potential to be exposed to pollutants through pathways such as ingestion, inhalation and dermal contact with soils, soil dust, and shallow groundwater and surface water, or by migration of ground gases into confined spaces. While people are exposed to various chemicals routinely in life, there are some hazardous chemicals that raise particular health concerns because of their widespread presence in the environment, their toxicity, and their capacity to magnify and accumulate in the environment and in people. The fact that they are widespread and many people come into contact with them also means that they have the potential to harm the health of large populations. Chemicals, or groups of chemicals, of major public health concern include air pollution, arsenic, asbestos, benzene, cadmium, dioxin and dioxin-like substances, inadequate or excess fluoride, lead, mercury and highly hazardous pesticides (WHO, 2020).
Interpretation for Assessment
- The assessment has been informed by Chapter 13 (Geology and Soils) and Chapter 19 (Road Drainage and the Water Environment) but has also considered the likelihood of human exposure to pollution after taking account of legislative frameworks, such as that afforded by the Environmental Protection Act 1990, Health & Safety legislation and standard environmental management practices. While exposure to pollution has been assumed as negative to health, effects have only been considered to be significant if widespread population exposure is considered likely or particularly vulnerable groups are affected.
Human Health Evidence Associated with Safety Associated with the Affected Road Network (HD9)
- Road traffic collisions are a direct cause of mortality, injuries and disability. Road traffic collisions also have a severe effect on mental health and are the leading cause of post-traumatic stress disorder (PTSD) in the general population (Kovacevic et al., 2020) with life-long health implications for individuals affected. The WHO predicts that road traffic collisions will become the fifth leading cause of death globally by 2030 (WHO, 2023b) and that they are currently the leading cause of death for children and young adults (aged 5-29 years) (WHO, no date).
- Changes to traffic movements and flows can also change people’s perceptions in relation to traffic safety, which can act as a barrier to travel, physical activity and social interaction (Anciaes et al., 2017). Commentary on road traffic accidents is provided in Chapter 2 (Need for the Scheme).
Interpretation for Assessment
- While the greater proportion of road collision fatalities are among car drivers, the fatality rate among motorcyclists, pedestrians and cyclists is substantially higher, indicating the greater vulnerability for these types of travellers. In most cases, fatalities among these types of travellers involve a collision with a car or other motor vehicles. Measures which help separate vulnerable travellers from motor vehicles have been assumed to be positive for health.
- The results of traffic collision analysis have informed the assessment. Significant positive health outcomes are judged to be likely if there is a substantial reduction in risk of serious injury and fatalities from collisions, particularly for motorcyclists, pedestrians and cyclists, whilst accessibility for these modes of travel is maintained or improved.
Human Health Evidence Associated with Flood risk (HD10)
- Flooding can result in injury and illness, and in extreme cases, death by drowning. Flooding can impact people’s wellbeing, psychosocial resilience, relationships and mental health, often over extended periods of time (Stanke et al., 2012; Public Health England, 2020).
- Direct impacts on flood storage and flow mechanisms have been reported in Chapter 19 (Road Drainage and the Water Environment).
Interpretation for Assessment
- As part of Scottish Planning Policy, any new development must remain flood free during any design flood event as well as not increasing flood risk in the surrounding areas. The human health assessment has considered whether flood risk would be improved and/or the likelihood of the proposed scheme in changing people’s perception of flood risk.
Assessment Reporting and Significance Criteria
- The DMRB LA 112 requires health outcomes to be reported according to the categories in Table 18.5.
Table 18.5: Human Health Outcome Categories – DMRB LA 112
|
Health Outcome Category |
Health Outcome Description |
|
Positive |
A beneficial health impact is identified |
|
Neutral |
No discernible health impact is identified |
|
Negative |
An adverse health impact is identified |
|
Uncertain |
Where uncertainty exists as to the overall impact |
- The assessment criteria for human health outcome categories in relation to sensitivity, magnitude and significance are outlined in paragraphs 18.2.64 – 18.2.71.
Assessment Criteria
Sensitivity Criteria
- The DMRB LA 112 states that ‘once the health profile of communities has been established, the sensitivity of a community/population to change shall be identified (supported with evidence).’ It goes on to state that the sensitivity shall be reported as low, medium or high. However, the DMRB LA 112 does not provide sensitivity criteria on which to base this judgement on. Therefore, sensitivity criteria from the IEMA guidance on determining significance for human health in Environmental Impact Assessment (Pyper et al., 2022a) have been used to guide the assessment. The criteria in the IEMA guidance use four categories of sensitivity (high to very low). Therefore, the criteria have been adapted to combine the very low and low sensitivity criteria into one. This allows for alignment with the DMRB LA 112 reporting requirement for sensitivity. The criteria used are set out in Table 18.6.
- Depending on the impact being assessed, some population groups may be more vulnerable to impacts than others. For example, young people and elderly people are considered more sensitive to poor air quality (Royal College of Physicians, 2018). Similarly, people in residential premises, schools, and places of worship are likely to be more sensitive to some impacts e.g. noise. For this assessment, vulnerable groups have been considered on a case-by-case basis.
Table 18.6: Criteria for Sensitivity of Population Groups (adapted from Pyper et al., 2022a)
|
Sensitivity level |
Indicative criteria for the population |
|
High |
High levels of deprivation (including pockets of deprivation);
|
|
Medium |
|
|
Low |
|
Magnitude Criteria
- For the assessment of human health, magnitude has been determined based on the potential for a change in health determinant and, where there is a pathway for this change in a health determinant to lead to a change to health status for a group or population, known as a health outcome. In the absence of criteria for determining magnitude in DMRB LA 112, this has been determined using the IEMA guidance (Pyper et al., 2022a) and professional judgement based on data gathered and the conclusions of the other chapters e.g. air quality. Table 18.7 provides the magnitude criteria included in the IEMA guidance.
Table 18.7: Criteria for Magnitude of Health Impacts (source: Pyper et al., 2022a)
|
Magnitude level |
Indicative criteria for the magnitude of change for health determinants on the population groups |
|
High |
|
|
Medium |
|
|
Low |
|
|
Negligible |
|
- Neither the DMRB guidance (LA 104 or LA 112) nor the IEMA guidance provide definitions for long-term, medium-term or short-term. The following timescales, applied in this assessment, have been defined using professional judgement and experience from similar projects:
- long-term: impacts lasting approximately ten years or more;
- medium-term: impacts which would last approximately three to ten years;
- short-term: impacts which would last approximately six months to three years;
- very short-term: impacts which would last up to six months; and
- transient: impacts lasting a matter of hours or up to a weekend.
Significance Criteria
- The judgement of significance involves the synthesis of information to determine whether health effects are important, desirable and/or acceptable in terms of public health. This assessment has been guided by the significance criteria from the IEMA Guide to Determining Significance for Human Health in Environmental Impact Assessment (Pyper et al., 2022a) as set out in Table 18.8. Similar to DMRB LA 104, the process for determining the significance of effect, as set out in the IEMA Guide to Determining Significance for Human Health in Environmental Impact Assessment (Pyper et al., 2022a), takes into consideration the sensitivity of the population and the magnitude of change.
- The matrix presented in Table 18.9 is based on the generic indicative EIA significance matrix provided in the IEMA guidance but has been adapted through the removal of the ‘very low’ sensitivity category, to align with the DMRB LA 112 sensitivity reporting requirement (as explained in paragraph 18.2.64 above). A matrix based on the IEMA guidance has been used in preference to the generic matrix provided in Table 3.8.1 of DMRB LA 104 for the following reasons:
- Table 3.8.1 of DMRB LA 104 differs from DMRB LA 112 in providing for five categories of sensitivity rather than three, meaning a greater modification of the matrix is needed to align with DMRB LA 112.
- DMRB LA 104 allows for the reporting of ‘neutral’ significance for negligible or minor magnitude impacts, which is not appropriate for some health determinants where there is no level below which an effect on a population can be observed, such as is the case of air pollution. Therefore, the IEMA guidance which applies the term ‘negligible’ has been adopted for this human health assessment. The term ‘neutral’ is only applied in this assessment where no change to a determinant is predicted.
- Similar to Table 3.8.1 in DMRB LA 104, where two significance categories are provided for a cell in Table 18.9, evidence has been provided to support the reporting of a single significance category.
Table 18.8: Criteria for Significance of Effect
|
Level |
Indicative criteria for the significance of effect |
|
Major (significant) |
|
|
Moderate (significant) |
|
|
Minor |
|
|
Negligible |
|
Table 18.9: Indicative Health Assessment Significance Matrix
|
Magnitude Sensitivity |
No change |
Negligible |
Low |
Medium |
High |
|
High |
Neutral |
Minor or negligible |
Moderate or Minor |
Major or Moderate |
Major |
|
Medium |
Neutral |
Minor or negligible |
Minor |
Moderate |
Major or Moderate |
|
Low |
Neutral |
Negligible |
Minor or Negligible |
Minor |
Moderate or Minor |
- Note that the initial assessment of potential impacts does not consider additional mitigation, only embedded mitigation as part of the design. The assessment of residual effects does consider additional mitigation and outlines the anticipated effects after all mitigation is taken into account.
Mitigation
- The approach to mitigation follows the hierarchical approach of avoidance and prevention, reduction, and remediation as set out in Table 3.5 of Chapter 3 (Overview of Assessment Process).
- DMRB LA 104 (Highways et al., 2020a, p.18) requires mitigation to be reported under two distinct categories:
‘1) embedded mitigation: project design principles adopted to avoid or prevent adverse environmental effects; and
2) essential mitigation: measures required to reduce and if possible offset likely significant adverse environmental effects, in support of the reported significance of effects in the environmental assessment.’
- The embedded mitigation measures outlined in Table 6.2 of Chapter 6 (The Proposed Scheme) and in each of the relevant topic chapters e.g. noise and vibration, have been taken into account prior to the human health impact assessment.
- Where negative impacts are predicted, or where opportunities to maximise health benefits are identified, recommendations for mitigation or enhancement have been put forward with further consideration of the community objectives. This will help to challenge the design against its ability to meet community objectives, with an assumption that this will help improve community wellbeing outcomes. Additional mitigation for human health impacts is considered as essential mitigation and is set out in Section 18.5.
Cumulative Effects
- Potential for cumulative effects of the proposed scheme, and those of the proposed scheme in combination with other reasonably foreseeable developments, are assessed in Chapter 21 (Assessment of Cumulative Effects).
Limitations to Assessment
- At the time of writing, the construction information available, including information relating to haul routes within temporary works areas and construction vehicle traffic, is indicative only and subject to change once the Contractor is appointed. Therefore, any impacts on health assessed in relation to construction traffic may be subject to a similar change.
- As noted in Chapter 1 (Introduction), the design of the proposed scheme may be refined, but will still be deemed to comply with this EIAR provided that such refinements to this design would be subject to environmental review to ensure that design refinements do not introduce new significant effects not reported in this EIAR or change the significance of effect reported in this EIAR from non-significant to significant.
- The health profile created for the communities has largely been based on data collection from secondary sources. Whilst this search has provided general information on vulnerable groups along the proposed scheme, the data gathered is high-level and not all specific cases have been captured. In particular, the assessment does not assess the health outcomes for individuals.
- Baseline data at a community level was not available for every human health indicator. No community level data was available on deaths from chronic obstructive pulmonary disease (COPD) or deaths from respiratory illness. It is considered that the absence of this baseline data would not significantly change the reported sensitivity of the communities.
- While consultation was received for the relevant EIA topic chapters which feed into the human health assessment, specific consultation data for the assessment were limited. No baseline data for the communities in the study area were received, however, it is considered that the desk-based sources have provided suitable data to inform the human health profiles. General consultation was undertaken as detailed in paragraphs 18.2.15 – 18.2.16, and it is considered that this consultation captured potential human health issues appropriately.
Baseline Conditions
Introduction
- This section sets out the baseline data gathered from the desk-based study used to establish baseline health profiles of the communities within the study area as well as baseline health determinants.
- The DMRB LA 112 provides a list of health indicator data to be collected from which to establish the baseline health profile. However, some data listed in LA 112 are not readily available from Public Health Scotland, therefore, alternative data have been provided. For example, data on the percentage of the community with respiratory disease/COPD) and deaths from respiratory disease could not be identified for the community study area.
- Where available, data have been provided for the data zones within which Birnam, Little Dunkeld, Dunkeld and Inver are located, however, where data were not available at such small area level, data from the Intermediate Zone of Luncarty & Dunkeld were used instead (see section 18.2 for more information on study areas). Health profile data are presented in Table 18.10 and described below.
Baseline Community Health Profile
- In the 2022 Scottish Census, the population of the Dunkeld and Birnam study area was 1,773 (Scotland’s Census, 2022a) accounting for approximately 1% of the wider population of Perth & Kinross (150,953) (Scotland’s Census, 2022b). Table 18.10 sets out health profile indicators. Approximately 7% of the Dunkeld and Birnam study area is income deprived, compared with 12% for Scotland as a whole. The population of the Dunkeld and Birnam community study area is older than average for Scotland. 14.3% of the population are children aged under 16 years, while 27% of the population is aged over 65 years, compared to the national average of 20%. Despite having a notably higher population of older people, the community has slightly lower proportions of its population limited a lot through disability or living with long-term health conditions, compared to the Scottish average. Asthma and COPD hospitalisations are lower than the regional and national averages. The community has a higher than average (for region and Scotland) proportion of its residents who reported good or very good health during the 2022 Census, and a lower than average proportion reporting bad or very bad health.
- Data for the Intermediate Zone of Luncarty & Dunkeld show significantly longer life expectancy for both males and females compared to the Scottish average, and the rate of premature deaths (aged under 75 years) is also better than average for Scotland.
- Causes of death from disease of the respiratory system (influenza, pneumonia, chronic lower respiratory diseases and asthma) in 2023, across the whole of Scotland, accounted for 6,953 deaths (approximately 11.0% of total deaths in Scotland), while deaths from these causes in the local authority area of Perth & Kinross accounted for 183 deaths (approximately 9.8% of deaths in Perth & Kinross) (National Records of Scotland, 2023). These data illustrate that respiratory illness is a less common cause of death in Perth & Kinross than in Scotland overall. However, no data are readily available at community study area level. Therefore, data on asthma and COPD hospitalisations and deaths under the age of 75 years have been collected to inform the understanding of the local health profile.
- There is limited mental health indicator data available at local level, therefore regional level data for the Perth & Kinross Council area have been used. There is a lower proportion of the population prescribed drugs for anxiety/depression/psychosis than the Scottish average, however, the suicide rate is higher than the Scottish average. The reason for this mismatch is not known from the available data but could reflect factors such as isolation and differences in access to appropriate mental health services.
- Based on the sensitivity criteria set out in Table 18.6, the general population health sensitivity of the Dunkeld and Birnam community study area is judged to be low. This reflects the relatively low levels of income deprivation, good general health, and relatively low levels of disability. However, the study area does have an older than average population who may require some care.
Table 18.10: Community Health Profile Data
|
Health Profile Indicators |
Dunkeld & Birnam (Community Study Area) |
Luncarty & Dunkeld (Community Study Area) |
Perth & Kinross (Comparator) |
Scotland (Comparator) |
|
Population aged under 16 years (%) (Scotland’s Census, 2022c; 2022d; 2022e) |
14.3 |
15.9 |
15.8 |
16.4 |
|
Population aged over 65 years (%) (Scotland’s Census, 2022c; 2022d; 2022e) |
27.0 |
23.0 |
21.6 |
20.0 |
|
Asthma patient hospitalisations (Age-sex standardised rate per 100,000) (2019/20 - 2021/22; 3-year aggregate) (Public Health Scotland, 2024a) |
Data not available |
29.6 |
52.9 |
68.4 |
|
COPD hospitalisations (Age-sex standardised rate per 100,000) (2020/21 - 2022/23; 3-year aggregate) (Public Health Scotland, 2024a) |
Data not available |
56.0 |
79.7 |
116.5 |
|
Incidence of COPD (age standardised rate per 100,000) (2020/21 – 2022/23) (Public Health Scotland, 2024a) |
Data not available |
Data not available |
84.9 |
83.1 |
|
Population with long-term health condition (%) (Scotland’s Census, 2022i; 2022j; 2022k) |
21.2 |
20.9 |
21.9 |
21.4 |
|
Population whose day-to-day activities are limited a lot through disability (%) (2022) (Scotland’s Census, 2022i; 2022j; 2022k) |
9.9 |
8.9 |
9.3 |
10.8 |
|
Population prescribed drugs for anxiety/depression/psychosis (%) (2021/22) (Public Health Scotland, 2024a) |
Data not available |
Data not available |
18.1 |
20.1 |
|
Deaths from suicide (16+ years) Age-standardised rate per 100,000 (2018-2022; 5-year aggregates) (Public Health Scotland, 2024a) |
Data not available |
Data not available |
22.5 |
17.5 |
|
Population reporting good or very good general health (%) (Scotland’s Census, 2022f; 2022g; 2022h) |
82.2 |
83.4 |
81.4 |
78.8 |
|
Population reporting fair general health (%) (Scotland’s Census, 2022f; 2022g; 2022h) |
12.7 |
11.48 |
13.1 |
14.2 |
|
Population reporting bad or very bad general health (%) (Scotland’s Census, 2022f; 2022g; 2022h) |
4.9 |
5.1 |
5.5 |
6.9 |
|
Life expectancy at birth (years) (females) (2017-2021; 5 year aggregate) (Public Health Scotland, 2024a) (*Perth & Kinross Council life expectancy data are for years 2020-2022 3-year aggregate rather than the 2017-2021 5-year aggregate.) |
Data not available |
84.3 |
82.5* |
80.7 |
|
Life expectancy at birth (males) (years) (2017-2021; 5-year aggregate) (Public Health Scotland, 2024a) (*Perth & Kinross Council life expectancy data are for years 2020-2022 3-year aggregate rather than the 2017-2021 5-year aggregate.) |
Data not available |
79.6 |
78.8* |
76.5 |
|
Deaths under 75 years (age standardised rate per 100,000) (2020 – 2022) (Public Health Scotland, 2024a) |
Data not available |
334.1 |
367.8 |
453.0 |
|
Population who are income deprived (%) (SIMD) (Scottish Government, 2020a) |
7.3 |
6.5 |
8.0 |
12.1 |
Baseline Health Determinants
Community, recreational and education facilities (HD1)
- Chapter 16 (Population - Land Use) identifies community land and assets located in Dunkeld, Little Dunkeld, Birnam and Inver. These include village halls, healthcare facilities, postal services, education facilities, and religious facilities. The location of these facilities is shown on Figure 16.1.
- Some of the facilities have been identified as serving multiple functions, as follows:
- Birnam Arts and Conference Centre (art centre, community centre, library, conference centre, Beatrix Potter Exhibition and café).
- Dunkeld & Birnam Recreation Club (outdoor recreation centre comprising two all-weather tennis courts, bowling green and a grass football pitch) and designated as Open Space.
- Royal School of Dunkeld (nursery and primary school and community education/adult education base).
- The community facilities within Birnam, Dunkeld and Little Dunkeld, with the exception of Dunkeld & Birnam Station, are located north of the A9 and there is no notable community severance, although there is only a single crossing point of the River Tay via Dunkeld Bridge to get between Dunkeld and Little Dunkeld. The small community of Inver lacks community facilities, therefore, residents are likely to travel to Little Dunkeld, Birnam and Dunkeld for facilities and local services, which means vehicular travellers must negotiate junctions onto and off of the A9. Pedestrians currently use an underpass under the A9 and previously used a pedestrian route via a wooden bridge across the River Braan, however, Core Path DUNK/63 providing access to the Inver road footway east of Inver Bridge is currently used as a diversion for the Braan footbridge, as it has been washed away and not yet reinstated. The underpass pedestrian route is relatively enclosed by trees and may be intimidating to some people, particularly at night. This may contribute to a degree of isolation or severance from community facilities for some groups in Inver.
- Access to public services and social infrastructure is a key determinant of health and wellbeing. The SIMD ‘Geographic Access to Services’ domain, which has 10 indicators relating to access, was used to evaluate baseline connectivity to services within the local community study area comprised of the 2011 data zones of S01012007 and S01012008 (see Table 18.3 for further details). SIMD access indicator descriptions are provided in Table 18.11.
Table 18.11: SIMD Access Indicator Descriptions and Ratings (Scottish Government, 2020b)
|
Indicator |
Data Zone S01012007 |
Data Zone S1012008 |
Comments |
|
Average drive time to a petrol station in minutes |
3.2 |
4.8 |
S01012007 ranks within the best 50% of data zones in Scotland (2nd quartile). S01012008 ranks within the worst 25% of data zones in Scotland (4th quartile). |
|
Average drive time to a General Practitioner (GP) surgery in minutes |
3.4 |
4.0 |
Both rank within the worst 50% of data zones in Scotland (3rd quartile). |
|
Average drive time to a post office in minutes |
2.6 |
4.5 |
S01012007 Ranks within the worst 50% of data zones in Scotland (3rd quartile). S01012008 ranks within the worst 25% of data zones in Scotland (4th quartile). |
|
Average drive time to a primary school in minutes |
2.7 |
4.4 |
S01012007 ranks within the best 50% of data zones in Scotland (2nd quartile). S01012008 ranks within the worst 25% of data zones in Scotland (4th quartile). |
|
Average drive time to a retail centre in minutes |
3.1 |
3.7 |
Both rank within the best 50% of data zones in Scotland (2nd quartile). |
|
Average drive time to a secondary school in minutes |
18.3 |
18.6 |
Both rank within the worst 25% of data zones in Scotland (4th quartile). Both also fall within the worst 10% of data zones in Scotland (90th percentile). |
|
Public transport travel time to a GP surgery in minutes |
9.4 |
12.3 |
Both rank within the worst 50% of data zones in Scotland (3rd quartile). |
|
Public transport travel time to a post office in minutes |
7.2 |
13.2 |
S01012007 ranks within the best 50% of data zones in Scotland (2nd quartile). S01012008 ranks within the worst 25% of data zones in Scotland (4th quartile). |
|
Public transport travel time to a retail centre in minutes |
8.7 |
12.1 |
S01012007 ranks within the best 50% of data zones in Scotland (2nd quartile). S01012008 ranks within the worst 50% of data zones in Scotland (3rd quartile). |
|
Percentage of premises without access to superfast broadband (at least 30Mb/s download speed) |
18% |
26% |
Both rank within the worst 25% of data zones in Scotland (4th quartile). |
- As indicated in Table 18.11, the communities within the S01012008 data zone fare comparatively worse in the majority of indicators for the access domain in Scotland overall. The average drive time to a secondary school in minutes is the worst ranked indicator for both data zones in the community study area when compared with the rest of the data zones in Scotland, ranking within the worst 10%. It should however be noted that the data zone covered for S01012008 covers an expansive area and contains small, isolated communities that are located some distance from Inver and Little Dunkeld and the location of the proposed scheme.
Landscape amenity and green/open space (HD2)
- Chapter 10 (Landscape) describes the landscape elements and features of the study area, which is characterised by the varied landscape of the Tay valley. Roads, including the existing A9 and A984, and the Highland Main Line railway run parallel to the River Tay and are the main built elements of the landscape, with the designed landscapes of Murthly Castle, Dunkeld House and The Hermitage oriented to take advantage of views to the Rivers Tay and Braan.
- Visual receptor locations (places where individuals and/or groups of people have the potential to be affected by views of the proposed scheme) within the study area largely comprise residential properties within the settlements of Birnam and Little Dunkeld, together with individual farmsteads and properties along the route corridor. In addition, there are a number of sites used for outdoor recreation and travel routes including roads, the Highland Main Line railway, and recreational walking and cycling routes, which pass through scenic areas.
- The existing A9 is a notable feature in many views across the Tay valley as it runs along the eastern edge of the valley floor, although established mature woodland areas provide some screening to/from the A9. The topography of the area generally limits views to within the valley itself, with the rising valley sides adjoined by gradually increasing hills to the east and west helping to screen more distant views into the area.
- The importance the local community place on protecting the landscape is evidenced by the Birnam to Ballinluig A9 Community Group’s community objective 2 for the proposed scheme as set out in Table 18.2.
- Public Health Scotland identifies that high quality open spaces and environments are ‘crucial building blocks of health and wellbeing’ (Public Health Scotland, 2024b). Public Health Scotland outlines various pathways by which open space helps to support good health and wellbeing. Open space provides opportunity for physical activity, for example, through outdoor recreation, which is important for physical and mental health. It is also an important asset for community development. This is evidenced in Dunkeld and Birnam where there are several community groups focused around local outdoor spaces, such as The Orchard (community orchard) and The Field (community growing project). There is good evidence that exposure to green space is associated with increased self-reported levels of mental health and wellbeing (Public Health Scotland, 2024b; Houlden et al., 2018). Green space is also important to health in the context of climate change and biodiversity as well as in providing urban cooling and reducing flood risk (WHO, 2023a).
- Several areas of green and open space are identified in Chapter 16 (Population - Land Use) and shown on Figure 16.1. These include Riverside Land (National Trust for Scotland), Dunkeld & Birnam Recreation Club (Community Facility), Beatrix Potter Garden, Jubilee Park, Birnam Play Area, Land by Little Dunkeld Manse (the site of Birnam Highland Games), Little Dunkeld Recreation Park, and Riverside Play Area. The communities of Dunkeld, Little Dunkeld, Birnam and Inver are surrounded by areas of forestry, riverside paths and hills. There are several trails which can be followed to access these areas on foot or by bike. However, the A9, combined with the Highland Main Line railway, limits the number of routes by which people from these settlements can access the green space to the south.
Healthcare facilities (HD3)
- Craigvinean Surgery is a GP practice located in Little Dunkeld. There is a dental practice and a chemist located on Bridge Street in Dunkeld, while the Rivendell House Care Home is located of Oak Road, Birnam. These healthcare facilities are shown on Figure 16.1 (excluding the chemist which is mentioned in Appendix A16.1 but is not included on Figure 16.1 as it is considered to be a business rather than a community asset).
- The nearest Accident & Emergency (A&E) department is at Perth Royal Infirmary, in Perth, some 22km from Birnam and Dunkeld via the A9. To the north there is the Pitlochry Community Hospital, which is an integrated healthcare facility that doesn’t have an A&E department but has a community ward with inpatient beds and various outpatient clinics. This is located approximately 18km north of Birnam and Dunkeld via the A9 and the GP may refer patients to this facility for its Community Care and Treatment Service, which delivers a range of services, including wound care, blood sample services (phlebotomy), chronic disease monitoring (including blood pressure checks), and suture and clip removal. The A9 therefore provides an important link to secondary healthcare services for residents in the local community study area.
Community identity, culture, resilience and influence (HD4)
- This determinant relates to the way people feel about their community, including opportunities to contribute to a positive community identity, sense of belonging and sense of control (Pyper et al., 2022b). Several of the community assets and land identified in Figure 16.1 relate to cultural and artistic activities.
- The Dunkeld & Birnam Tourist Association has a website to promote Dunkeld and Birnam to visitors. It includes insights from individuals representing different interests in the local community (Dunkeld & Birnam Tourist Association, no date). The website highlights several aspects of relevance to community identity and culture. Some of these are outside of the study areas for Chapter 16 (Population - Land Use) and Chapter 17 (Population - Accessibility), but are valued by the Birnam and Dunkeld community, including:
- outdoor recreational activities (for example mountain and trail biking, dog walking, hiking, paddleboarding, climbing and fishing);
- local food and community growing (with reference to The Field community growing project and The Orchard community orchard);
- arts and music (with reference to music venues, societies and festivals, the Birnam Arts Centre and local art galleries);
- local landmarks and places such as Dunkeld Cathedral, the Hermitage; Stanley Hill; Tay Forest Park; Birnam Wood; and Neil Gow Oak ‘The Fiddler Tree’;
- play areas and activities for children;
- natural heritage, including the Lowes nature reserve; and
- local history, with reference to the Battle of Dunkeld in 1689, the Thomas Telford designed Dunkeld Bridge, genealogical resources in the Community Archive, and the Birnam Highland Games which have taken place annually for over 150 year).
- During the A9 Co-Creative Process (see Section 18.2), the Community Objectives 2 and 7 reflected the importance that the Birnam to Ballinluig A9 Community Group placed on preserving green spaces and a sense of community identity, local pride and culture (see Table 18.2).
Spatial characteristics of the transport network and usage (HD5)
- Both the A9 and the Highland Main Line railway form the south-western edge of the settlements of Little Dunkeld and Birnam. A baseline description of the transport network is set out in Section 17.3 (Chapter 17: Population - Accessibility). It describes the baseline with regard to core paths, public rights of way and other routes and facilities for walkers, wheelers, cyclists and horse riders. It also presents information on bus services and bus stops. This includes two bus stops on the A9 itself (one on the northbound side, the other on the southbound side near Rose Cottage, Inver). Bus users would have to cross the A9 to get between Inver and the southbound bus stop and to get between Dunkeld and Birnam and the southbound bus stop.
- The baseline routes and crossing points of the A9 are shown on Figure 17.1. While the A9 effectively bypasses Dunkeld and Birnam, its alignment does separate Inver from Little Dunkeld. As noted above, there is a pedestrian route via an underpass of the A9 and a diversion via Core Path DUNK/63, for the Braan footbridge that has not yet been reinstated, currently used as a way which pedestrians could get between these settlements. This is crossing point reference CP04 in Chapter 17 (Population - Accessibility).
- Road access to the Birnam and Dunkeld Railway Station is directly off the A9, while pedestrian access is via Birnam Glen, which is part of National Cycle Network Route (NCR) 77. This route crosses the A9 via an underpass (crossing point reference CP03 in Chapter 17: Population - Accessibility). The access from Birnam Glen (NCR 77) to the station itself involves steps and so is not suitable for users of wheelchairs and would be inconvenient for pushchair users and cyclists. Dunkeld & Birnam Station is a shared railway station serving both towns, situated on the Highland Main Line railway. Details on existing train services are provided In Table 17.9b of Chapter 17.
- Table 17.7 in Chapter 17 (Population - Accessibility) identifies a total of six crossing points of the A9 in the study area applied for the accessibility assessment. In addition to crossing points CP03 and CP04 described above, there are two others which are grade separated from the A9. CP06 is where the NCR 77 crosses under the A9 Jubilee Bridge on the left bank (refers to the perspective of the viewer when facing downstream) of the River Tay, while CP07 is where Path 35 (a core path and part of the Inver Path walking route) crosses under the A9 Jubilee Bridge on the right bank of the River Tay. Crossing points CP01 and CP02 are both at-grade with no dedicated facilities to support pedestrians or cyclists. Baseline traffic on the A9 at these locations was recorded at between 16,500 and 17,500 vehicles per day (24 hour annual average daily traffic (AADT)) which is at a level likely to deter people from crossing at these points. CP01 relates to a local path, while CP02 relates to a core path and public right of way. Both of these locations are for rural routes, so most likely to affect people on recreational journeys rather than causing baseline severance for people accessing community facilities.
Air quality (HD6)
- The links between air pollution and health effects are well established (refer to paragraphs 18.2.40 – 18.2.47). The main pollutants from vehicle emissions are particulate matter and oxides of nitrogen (NOx). Air quality standards are set to provide an acceptable level of health protection. Chapter 8 (Air Quality) sets out the legislative and baseline context for air quality.
- There are no Air Quality Management Areas (AQMA) within the local community study area. The Perth and Crieff AQMAs lie approximately 13km and 26km, respectively, outside of the air quality study area and are not considered to be within influence of the proposed scheme (refer to Chapter 8 (Air Quality) for more information).
- No baseline exceedances of the respective NO2, PM10 and PM5 Air Quality Objectives are predicted at human health receptor locations in the base year (2023) or for the opening year (2036) in the air quality study area (see Section 8.3 of Chapter 8 (Air Quality)), which falls within the local communities study area. This indicates that baseline air quality in the local study area is considered acceptable for human health.
Noise and the ambient noise environment (HD7)
- Section 15.3 of Chapter 15 (Noise and Vibration) presents the noise baseline with respect to road traffic noise. Appendix 15-2 (Baseline Noise Survey) of Chapter 15 provides further details on the noise environment for the local communities and Figure 15.2 shows the baseline noise monitoring locations.
- The baseline noise monitoring locations and noise levels (listed in a south to north direction) are presented in Table 18.12. Note that at The Old Bakehouse and St Catherine’s Cottage locations the measurements were taken 1m away from the property façade and therefore included reflections from the building. WHO guidance is based on free-field levels (i.e. not including reflections from the building in question), therefore t a reduction of 2.5dB (the industry standard correction for façade to free-field for road traffic noise) has been used to provide the free-field levels.
Table 18.12: Baseline Noise Levels
|
Measurement Location |
Baseline Lden (dB(A)) |
|
Rowan Cottage, Birnam |
59.0 |
|
Hollybank, Perth Road, Birnam |
55.7 |
|
St Catherine’s Cottage, Birnam |
60.9* |
|
Oakbank, Birnam |
56.9 |
|
The Old Bakehouse, 12 Birnam Terrace, Birnam |
50.6* |
|
6 King Duncan’s Place, Birnam |
63.6 |
|
Braeknowe, Birnam |
60.6 |
|
Caileagan, Little Dunkeld |
58.3 |
|
Craigview, Inver |
64.0 |
- Road traffic noise from the existing A9 is a primary component of the baseline noise climate at all noise monitoring locations, with birdsong also heard at most locations. The average noise exposure recorded exceeded the WHO recommended level of 53dB Lden or less at all locations except one (The Old Bakehouse). Noise annoyance is subjective and is dependent upon individuals’ sensitivity to noise exposure. The noise exposure indicated in Chapter 15 and Appendix 15-2 shows that there is the potential for the current traffic noise levels to be associated with sleep disturbance. Residents of properties that are near to the A9 have the most potential to experience these outcomes.
Sources and Pathways of Potential Pollution (HD8)
Surface water quality
- Chapter 19 (Road Drainage and the Water Environment) identifies 16 watercourses that have all been scoped into the water quality assessment. Notable water features are the major watercourses the River Tay and River Braan, both of very high water quality. There are thirteen watercourses of medium water quality and one watercourse of low water quality.
- Chapter 13 (Geology and Soils) has noted one unknown status surface water fed private water supply within the study area. Details regarding the current quality of this supply are unknown.
Groundwater quality
- As outlined in Chapter 13 (Geology and Soils), the groundwater in the Bankfoot aquifer is described as generally weakly mineralised, with near neutral to alkaline pH values and high nitrate and elevated phosphate concentrations were recorded across aquifer units. The study area lies within a groundwater Drinking Water Protected Area. The southern extent of the study area, where the Isla and Lower Tay Sand and Gravel aquifer and Bankfoot aquifer are present, is classed a Nitrate Vulnerable Zone (NVZ) by the Scottish Government under the European Commission’s Nitrates Directive 91/676/EEC.
Chapter 13 (Geology and Soils) noted that there are two active groundwater fed (borehole) private water supplies and one active spring fed private water supply within the study area. Details regarding the current quality of these supplies are unknown but Chapter 13 does note that no change to existing groundwater pathways to residential occupants/buildings/services is predicted.
Land Contamination
- As outlined in Chapter 13 (Geology and Soils), seven potential sources of land contamination have been identified on-site (within the compulsory purchase order boundary) and a further ten potential sources of land contamination have been identified off-site. The on-site potential sources of contamination include the existing A9, potentially infilled ground (a curling pond and a gravel pit) and historic tanks which have the potential for localised leaks and spills to have occurred throughout their lifetime.
- The off-site potential sources of contamination comprise industry (e.g. factories or garages), potentially infilled ground (quarries and pits), utilities such as sewage works, gas works, and Ladywell Landfill. Further information on each potential source of land contamination is provided in Appendix A13.1 (Land Contamination Supporting Information) and locations are provided in Figure 13.3. Potential human health receptors to land contamination include construction workers, adjacent residents/workforce, maintenance and landscape workers and future road users. Risks for human health are discussed in paragraphs 18.2.52 – 18.2.53 of Section 18.2.
- Ground investigations, including the chemical laboratory analysis of soils and groundwater samples, were conducted to support the scheme design.
Safety associated with the affected road network (HD9)
- As set out in Chapter 2 (Need for the Scheme), one of the scheme objectives is to improve safety for motorised and non-motorised users by reducing accident severity and reducing driver stress. When the severity of recorded Road Traffic Collisions along the length of the A9 between Perth and Inverness is compared with National Averages for Single and Dual Carriageway standard between 2015 and 2022, the A9 is noted to have a higher proportion of Fatal and Serious recorded collisions.
- The majority of accidents on the A9 occur along sections of single carriageway, and generally near to junctions. The wider Dunkeld area (Pass of Birnam to Ballinluig) has been identified as a particular area of concern. Of high concern is the identified cluster at the immediate proximity of the staggered A9, A923 and A822 junction which provides access to Dunkeld and neighbouring settlements. At these junctions there have been five Serious collisions and eight Slight collisions.
- In September 2024 there was some consultation undertaken for the proposed scheme with children and young people from Royal School of Dunkeld, Pitlochry High School and Breadalbane Academy. Safety concerns were a common theme in the responses from children and young people, which included concerns about crossing the A9 as a pedestrian. One child from the Royal School of Dunkeld reported the following: ‘I see lots of car crashes on the A9 and it’s really scary. There was one car on its roof. I don’t like seeing this’. This is illustrative of the effects on mental wellbeing that witnessing traffic collisions can have on people.
Flood risk (HD10)
- Section 19.3 of Chapter 19 (Road Drainage and the Water Environment) describes the baseline with regard to fluvial flood risk as well as flood risk from other sources. The chapter identifies a number of locations where residential properties (139-159 in total) and other built assets (including a school, static caravans and a sewage treatment works) are at risk from flooding from principal watercourses in a one in two hundred year plus allowance for climate change flood event (the flood probability standard against which the proposed scheme is assessed). It also identifies several locations at risk of pluvial flooding. Reference should be made to Chapter 19 and its relevant appendices for further information on flood risk and how impacts from flooding are predicted and assessed.
- Paragraphs 18.2.59 – 18.2.61 outline a number of ways by which flooding can affect human health, including long term mental health impacts following the experience of flooding.
Potential Impacts and Effects
Introduction
- As outlined in Section 18.2, the assessment has used output from the relevant EIA topic chapters, a literature review and desk-based analysis to help determine the potential for direct and indirect human health effects as a result of the proposed scheme. Potential impacts to health determinants and health outcome effects are assessed for the construction and operation phase. A summary of the potential construction and operational effects is provided in Table 18.13 and Table 18.14 respectively. These are the population health effects which would be considered likely in the absence of any additional mitigation. The sensitivity, magnitude and significance have been determined through professional judgement and the application of the criteria set out in Tables 18.6, 18.7, 18.8 and 18.9.
Potential Construction Impacts and Effects
Community, Recreational and Education Facilities (HD1)
- Section 16.4 of Chapter 16 (Population - Land use) identifies potential physical land-take from community land and assets. None of the potential construction impacts identified in Chapter 16 (Population - Land use) appear likely to reduce the range and function of community, recreational and educational facilities that serve the community, although some reduction in accessibility is predicted for the Hermitage. It is judged that these impacts are more relevant to determinants HD4 and HD2 respectively. The main potential construction impact that may affect the health determining role of community, recreational and education facilities is whether there is construction disruption to the extent that some people would be dissuaded from accessing and using these facilities. Taking into account the location of community facilities, as indicated on Figure 16.1b, the main facility where there is potential for such an impact is the Dunkeld & Birnam Recreation Club, where the access is via a lane called Little Dunkeld which is within the red line boundary to the north of the proposed Dunkeld Junction Roundabout. There is potential for this access to be disrupted at least on an intermittent basis during construction of earthworks associated with the junction embankment, drainage works and tie-ins to the new junction. Any occasional disruption to Little Dunkeld Lane has potential to dissuade use of Dunkeld & Birnam Recreation Club with an associated reduction in social interaction and physical activity. It is expected this would affect a small minority of the population in the local area in the short-term. This has potential to affect the quality of life of people who use the facility and may affect a minor change in morbidity from reduced physical activity.
- The sensitivity of the general population is low, but the vulnerable group population, which may include children and the elderly who may depend on the recreation facilities, is high. This high sensitivity reflects the importance of physical activity for older people’s mobility and the importance of play for children’s health and wellbeing. A Moderate negative potential significance of effect has been applied for vulnerable groups on the basis that there is clear scientific evidence as to the benefits of physical exercise to health and wellbeing, that a short term duration could span a key developmental stage in the life of a child, and that having opportunities to take part in play, recreation and sport is a national priority.
Landscape Amenity and Green/Open Space (HD2)
- Construction activities associated with the proposed scheme would result in temporary adverse landscape impacts. The most significant negative landscape and townscape impacts during the construction period would be likely to occur where major structures and junctions and associated earthworks are being constructed and where the scheme interfaces with the existing townscape (see Chapter 10 (Landscape) for further details). Significant visual impacts have also been identified, with likely visual impacts on people using buildings and outdoor locations, including paths, nearby to the construction works (see Chapter 11 (Visual) for further details). Section 17.4 of Chapter 17 (Population - Accessibility) identifies potential significant impacts on access to outdoor areas through disruption, in the absence of mitigation, including temporary severance and realignment of the paths. However, these potential impacts are described in general terms as they will depend on detail and timing of activities undertaken by the Contractor which are not available at this time. Section 16.4 of Chapter 16 (Population - Land use) identifies potential impacts on community land, which includes some physical land-take of minor magnitude from Little Dunkeld Park and War Memorial, Riverside Land and The Hermitage, and negligible magnitude from Land by Little Dunkeld Manse and Dunkeld & Birnam Recreation Club. These areas are locations where people can currently access green/open space. The potential land-take from areas of community land predicted would have a negligible scale of impact on availability of green space to the local community due to the number and size of alternative areas of green space in and around the local community study area.
- It is anticipated that construction works would reduce the sense of tranquillity for people nearby the construction activities. However, although construction works may dissuade use of paths and amenities directly impacted in the short term, beyond the main construction activities the visual intrusion would be less and would affect a small minority of the population. Additionally, people would have access to alternative travel networks and areas of green space that are outside of the impacted areas to access landscape amenity areas. Considering the alternatives areas for landscape amenity available in the local area, and the small minority of the population affected, the magnitude of impact is considered to be low. It is not anticipated that any specific vulnerable groups would be affected by the predicted impacts, therefore, the health sensitivity is also judged to be low. As a result, the potential significance of effect is judged to be minor negative.
Healthcare Facilities (HD3)
- Traffic diversions and associated impacts on vehicle travellers during construction of the proposed scheme are not fully known at this stage. While it is assumed that vehicle access for emergency services would be provided at all times, there is a risk of delays for people needing to travel to hospital appointments via the A9 and traffic congestion may increase journey times in the short-term. There would be an overnight closure of Birnam Glen Road during construction of the Birnam Glen and Inchewan Burn Bridge which would result in temporary disruption for vehicles and WCH. Train cancellations are also anticipated for three to four days at a time during some periods of the construction works (such as construction of the proposed pedestrian underpass) which would disrupt use of the train network and require people to find alternative transports modes during these periods.
- There is potential for disruption of access for people seeking healthcare facilities in Birnam, Little Dunkeld and Dunkeld. In particular, Craigvinean Surgery is accessed via Little Dunkeld Lane where there is potential for access to be disrupted at least on an intermittent basis during construction of embankment earthworks, drainage works and tie-ins to the proposed Dunkeld Junction Roundabout. Although access to healthcare facilities would be retained, there is a risk of occasional delays for some of the population in the local area in the short-term. Ambulance services (and the recipients of their care) are particularly sensitive to delays in response times. Disruption could also have a wider effect on healthcare services for people in the area through people arriving late or missing their appointments, reducing the efficiency of healthcare services for patients. Those who are most likely to be affected are those seeking access to the hospitals via the A9 or railway, and those living in isolated communities to the south of the A9 who would be required to cross the proposed scheme in order to access healthcare facilities (i.e. Craigvinean Surgery, the dental practice and the chemist in Dunkeld).
- The sensitivity of the general population is low, but the vulnerable group population which may include people in poor health who may depend on the healthcare facilities is high. This high sensitivity reflects the importance of retaining access to healthcare facilities for those who are more vulnerable and may require more frequent access to facilities. A Moderate negative potential significance of effect has been applied to vulnerable groups on the basis that the disruption of access through temporary severance and diversions may present a barrier for those reliant on services accessed via those affected sections of the travel network. Vulnerable groups, such as people in very poor health or who have a long term health condition, may already face more access barriers compared to the general population and therefore be more sensitive to access changes.
Community Identity, Culture, Resilience and Influence (HD4)
- As explained for HD1, disruption of access for community facilities has the potential to dissuade use of those facilities, with an associated reduction in social participation, interaction and, consequently, support. In particular, the impact on access to the Little Dunkeld Park and War Memorial may have particular effects on community identity and culture. Changes to landscape amenity (HD2) and the noise environment (HD7) are anticipated, which may dissuade use of paths and amenities directly affected by the construction works with an associated reduction in social interaction and physical activity. This disruption to the community during construction, particularly through impacts from noise and views of the construction works, is expected to affect a small minority of the population in the local area in the short-term and could result in negative mental health outcomes through social isolation, annoyance and impacts to tourism businesses, reducing community resilience.
- The community objectives make clear that the community is concerned about protecting the scenic beauty and natural heritage of the area, which also generate important tourism revenues. Therefore, the general population of Birnam and Dunkeld are likely to have an awareness of and be interested in the outcomes of the proposed scheme and many people are likely to feel anxiety due to the uncertainty surrounding the impacts of the proposed scheme. However, this is likely to be somewhat alleviated through the early and continued community engagement.
- The magnitude of change is considered to be low, as the carriageway is already a prominent feature of the community and although the majority of the changes are long-term, adverse influences would gradually decline as there is adaptation to changes in views and increased screening as planting matures. The changes for health outcomes relate to minor effects on mental health related morbidity and quality of life. The sensitivity of the vulnerable group population is high and associated with those who have strong feelings that their community would be largely changed, whether for better or worse, as a result of the proposed scheme. People living in homes with direct views of the proposed scheme may also be particularly sensitive as there would be a low capacity to adapt.
Spatial Characteristics of the Transport Network and Usage (HD5)
- Traffic diversions and associated impacts on vehicle travellers during construction of the proposed scheme are not fully known at this stage, although, there would be an overnight closure of Birnam Glen Road during construction of the Birnam Glen and Inchewan Burn Bridge which would result in temporary disruption for vehicles and WCH.
- Disruption of access in the vicinity of the proposed scheme could impact the transport network in the area. Particularly vehicle users of the A9 (including public transport), train users accessing Dunkeld & Birnam Station, and WCH using paths within the immediate vicinity of the proposed scheme. Those who are most likely to be affected are those travelling via the A9, those using the train station and those living in isolated communities to the south of the A9 who would be required to cross the proposed scheme in order to access facilities located in Little Dunkeld, Dunkeld and Birnam and further afield.
- The disruption anticipated as a result of the construction of the proposed scheme includes temporary severance and diversions (this is described further in Chapter 17 (Population - Accessibility), traffic congestion, and train cancellations, which are anticipated for three to four days at a time during some periods of the construction works (such as construction of the proposed pedestrian underpass). More detailed assessment of the Dunkeld & Birnam Station is found within Chapter 16 (Population - Land Use). This could lead to socioeconomic and social impacts through people having to find alternative routes, arriving late to work, school or other commitments.
- The sensitivity of the general population is low as there is a higher capacity to adapt and impacts are focussed on the vicinity of the proposed scheme. However, the vulnerable group population, which may include people who are dependent on cars, such as people who are disabled and children and parents going to school, is high. This high sensitivity reflects the importance of the A9 and railway in accessing facilities in the wider area, particularly for those who are more vulnerable and may require more frequent access to facilities, such as children travelling to and from school daily and commuters. A Moderate negative potential significance of effect has been applied to vulnerable groups on the basis that the disruption of access through temporary severance and diversions may present a barrier for those reliant on those affected sections of the travel network. Vulnerable groups, such as children and people who are disabled, may already face more access barriers compared to the general population and therefore be more sensitive to disruption of the transport network.
Air Quality (HD6)
- Chapter 8 (Air Quality) has predicted that impacts from dust deposition during construction would not be significant, with any potential dust impacts being of negligible or low risk to human health. On the basis of the findings in Chapter 8 (Air Quality) it can be assumed that there would be a negligible magnitude of change for the general population as dust impacts would be very short term and relate to a minor change in quality of life for most people. However, for the vulnerable group population, which may include people in poor health or those with respiratory conditions, the magnitude of change is judged to be low on the basis that they may be susceptible to a minor change in morbidity or moderate change in quality of life if they are more concerned. Consequently, the potential significance of effect for the general population is considered to be negligible negative and, for more sensitive, vulnerable groups, minor negative.
Noise and the Ambient Noise Environment (HD7)
- Chapter 15 (Noise and Vibration) has predicted significant construction noise impacts for several receptors (see Section 15.4 and Table 15.17 for further information on the source of construction noise and locations most affected). In terms of population health, these impacts are predicted to be of medium scale, affecting a major change in quality-of-life effect for a large minority of the population in the short-term. The general population is judged to have medium sensitivity to noise on the basis that many of those exposed would be in residential properties or wanting to enjoy the outdoor natural heritage of the area. Vulnerable groups may include those with ASD (autism spectrum disorder) or who have mental health conditions, or shift workers trying to sleep during the day, who are more likely to have a high sensitivity towards noise. On this basis, the effects of construction noise are judged likely to be of Moderate negative significance for the general population and Major negative significance for vulnerable groups.
Sources and Pathways of Potential Pollution (HD8)
- Chapter 13 (Geology and Soils) provides an assessment of risks from pollution and contaminated materials in soils and groundwater and potential pathways to human health receptors (i.e. people).
- The chapter identifies that the two private water supplies identified are not at risk of water quality impairment due to accidental spillage. Therefore, there is limited likelihood of human health exposure to potential pollutants entering groundwater for the population. Direct interaction is expected between construction of the proposed scheme and areas of land potentially impacted by land contamination. This interaction could lead to indirect impacts to human health during construction, associated with the potential ingestion, inhalation and dermal contact of any windblown soil dust and fibres arising from excavations and stockpiles of excavated materials.
- Whilst limited evidence of significant contamination was identified within the soils within the likely areas of soil disturbance during construction, Chapter 13 predicts a pre-mitigation magnitude of impact as minor negative for residential, open space, commercial and road human health receptors. For Chapter 13, this culminated in a pre-mitigation significance of effect of Moderate for residential, open space and commercial/industrial receptors (very high, high and medium sensitivity respectively) and slight for road users.
- Post construction, the chapter identifies the pre-mitigation significance of effects as Moderate for adjacent residential receptors, slight for open space and commercial/industrial receptors, and neutral for road users via the indirect exposure pathway associated with the potential ingestion, inhalation and dermal contact with any windblown soil dust and fibres arising from any exposed soils retained within scheme.
- The assessments summarised above from Chapter 13 are based on significance for individual receptors prior to any mitigation, whereas this assessment considers the potential impacts on population health. In terms of population health, the magnitude of health impact for the general population is judged to be low. This is based on information in Chapter 8 Air Quality which identifies a short-term negligible or low risk of dust impacts on human health receptors (see above under HD6), suggesting a low likelihood of exposure for the general population. The health sensitivity of the general population in the local study area is judged to be low during construction. This indicates minor negative potential significance of effect for the general population. There is a suggestive relationship between changes resulting from the proposed scheme and health outcomes when considered in the context of baseline exposure to various contaminants over lifetimes of individuals within the population.
- The vulnerable group population is expected to be those residents and users of open spaces in close proximity of the proposed scheme who are likely to be more conscious of the works and more concerned about potential health risks as a result. The sensitivity of the vulnerable group is judged to be medium. Since these groups would be closer to the works, the magnitude of health impact is also judged to be medium. This is based on a low risk of exposure in the short term to dust (identified in Chapter 8 Air Quality). This would indicate a Moderate negative potential significance of effect for vulnerable groups prior to any additional mitigation.
Safety Associated with the Affected Road Network (HD9)
- Disruption of the transport network as described under HD5 could have a wider effect on people in the area through psychological impacts (frustration, annoyance and stress due to route uncertainty) and safety concerns for active travellers commuting or recreational WCH. Temporary diversions of pedestrians and cyclists may increase the likelihood of collisions with traffic if not appropriately managed, increasing the risk of injury or death. The presence of construction works could also result in a reduction in perceived safety which could adversely affect social wellbeing, particularly if parents are more reluctant to allow their children outside to play or walk/cycle to school and other destinations. The magnitude of these road safety improvements is judged to be medium. While the impacts relate to mortality or changes in morbidity (fatalities and severe injuries and trauma from road traffic collisions) the changes are deemed likely to affect a small minority of the population in the short-term. The significance of unmitigated effect is judged to be Major negative.
Flood Risk (HD10)
- The flood risk assessment (FRA) (Appendix A19.2) identifies that there is a risk to life from flooding to those working on site, and the construction works also have the potential to impact the existing risk to life from flooding beyond the construction site. The FRA identifies potential adverse impacts on flood risk posed by temporary earthworks, temporary drainage, works within or adjacent to watercourses and general site activities, such as location of site compounds and storage areas and work traffic. Health effects from flood risk during construction include risk to life and psychological trauma in the event of an actual flood event, as well as the risk of anxiety and concern among local residents who may be concerned that construction activities could increase flood risk or reduce flood protection in the area.
- The sensitivity in the general population to this risk is expected to be low but may be medium among residents who have previously experienced flooding or are in the properties with baseline flood risk. The health magnitude is judged to be low as it would relate to occasional events affecting a minority of the population in the local study area. Consequently, the significance of effect is determined to be minor negative for both the general population and vulnerable groups.
Summary of Potential Construction Impacts
- Table 18.13 provides a summary of the potential impacts on health determinants and likely significance of effect for health outcomes during construction prior to any additional mitigation.
Table 18.13: Construction Summary – Potential Effects on Health and Wellbeing Determinants and Likely Health Outcomes
|
Health Determinants |
Sensitivity |
Potential Magnitude |
Potential Significance |
|
HD1: community, recreational and education facilities and severance/separation of communities from such facilities |
Low (general population) High (vulnerable groups) |
Low Low |
Minor negative Moderate negative |
|
HD2: landscape amenity and green/open space and severance/separation of communities from such facilities |
Low (general population and vulnerable groups) |
Low |
Minor negative |
|
HD3: healthcare facilities and severance/separation of communities from such facilities |
Low (general population) High (vulnerable groups) |
Low Low |
Minor negative Moderate negative |
|
HD4: community identity, culture, resilience and influence |
Low (general population) High (vulnerable groups) |
Low Low |
Minor negative Moderate negative |
|
HD5: spatial characteristics of the transport network and usage in the area |
Low (general population) High (vulnerable groups) |
Low Low |
Minor negative Moderate negative |
|
HD6: air quality |
Low (general population) High (vulnerable groups) |
Negligible Low |
Negligible negative Minor negative |
|
HD7: noise and the ambient noise environment |
Medium (general population) High (vulnerable groups) |
Medium Medium |
Moderate negative Major negative |
|
HD8: sources and pathways of potential pollution |
Low (general population) Medium (vulnerable groups) |
Low Medium |
Minor negative Moderate negative |
|
HD9: safety associated with the existing affected road network |
High (vulnerability of WCH to road traffic collisions) |
High |
Major negative |
|
HD10: flood risk |
Low (general population) Medium (vulnerable groups) |
Low Low |
Minor negative Minor negative |
Potential Operational Impacts and Effects
Community, Recreational and Education Facilities (HD1)
- Section 16.4 of Chapter 16 identifies potential physical land-take from community land and assets. None of the potential land-take impacts identified in Chapter 16 appear likely to reduce the range and function of community, recreational and educational facilities that serve the community. The proposed scheme provides for better connectivity via the A9 or across the A9, which would reduce baseline severance. The baseline severance related more to the relatively small population in the local study area in communities south of the A9 who are required to cross it to access facilities in Little Dunkeld, Dunkeld and Birnam. Therefore, the magnitude of impact is predicted to be low due to the small minority of the population likely to experience improved access to local facilities.
- Some vulnerable groups (disabled and children) may benefit from accessibility improvements (see assessment below for HD5) which may improve their access to community, recreational and education facilities. For example, if needing to travel by train, bus or via the WCH provision. However, it is considered that there would have been limited separation from facilities in the baseline so again, the magnitude of impact from the proposed scheme is judged to be low. The significance of effect is judged to be minor positive for the general population in the local study area and vulnerable groups. Some individuals are likely to benefit from the proposed scheme in terms of access to community facilities, but this is likely to result in a slight change to the population health baseline and marginally contribute positively to mental wellbeing.
Landscape Amenity and Green/Open Space (HD2)
- There are anticipated to be significant landscape and visual impacts as a result of an increased prominence of road infrastructure in the landscape/townscape and loss of defining features of the area in the long-term (see Chapter 10 (Landscape) and Chapter 11 (Visual) for further details). By the summer, 15 years after the proposed scheme opening, mitigation – mostly in the form of design choices, retention of existing vegetation and provision of new woodland and vegetation planting – would reduce the residual effects for all but one of the building and outdoor locations. The exception being at Dunkeld & Birnam Station where, although mitigation would reduce impacts, the reduction would not be to an extent that the significance of the residual effects anticipated would reduce. However, there are three buildings and five outdoor locations where people would continue to experience significant visual impacts, primarily affecting residents, walkers, cyclists and users of Dunkeld & Birnam Station in the summer 15 years after opening. Chapter 17 (Population - Accessibility) identifies potential disruption to access to several outdoor areas due to disruption of some paths (severance and realignments).
- From a human health perspective, potential land-take from areas of community land (Little Dunkeld Park and War Memorial, Dunkeld & Birnam Recreation Club, Land by Little Dunkeld Manse, Riverside Land and The Hermitage) identified in Chapter 16 (Population – Land Use) would have a negligible scale of impact on availability of green space to the local community due to the number and size of alternative areas of green space in and around the local community study area. This includes land available for public use post construction within the Compensatory Flood Storage Area near Inver. Therefore, it is not considered likely that people would be prevented from visiting outdoor spaces and there are several alternative locations in the community study area that would remain accessible.
- Considering the small scale of impact, the small minority of the population affected and the alternatives areas for landscape amenity available in the local area, the magnitude of impact is considered to be low. It is not anticipated that any specific vulnerable groups would be affected, therefore, the health sensitivity is also judged to be low for vulnerable groups. Consequently, the significance of effect is determined to be minor negative.
Healthcare Facilities (HD3)
- The proposed scheme would improve travel time and journey reliability on the A9 which would reduce the likelihood of missing appointments and provide more efficient routes for emergency services which could contribute to improved survival rates for certain emergency health conditions. The improved paths for WCH would also support safer and more convenient active travel modes to access healthcare facilities.
- The sensitivity of the general population is low, but the vulnerable group population, which may include people in poor health who depend on the healthcare facilities, is high. This high sensitivity reflects the importance of access to healthcare facilities for those who are more vulnerable and may require more frequent access. A Moderate beneficial potential significance of effect has been applied to vulnerable groups on the basis of the improvement of access, reliability and safety of access routes, either via the A9 or paths for WCH, to healthcare facilities.
Community Identity, Culture, Resilience and Influence (HD4)
- Improvements to pathways and the accessibility of the train station through the proposed scheme have the potential to increase uptake of active travel and allow more people to have better access to the public transport network. This can encourage physical activity, social interaction and allow participation from more members of the community. This has the potential to reduce negative mental health outcomes associated with social isolation and increase community resilience.
- The sensitivity of the vulnerable group population is high and associated with those who have strong feelings that their community would be largely changed, whether for better or worse, as a result of the proposed scheme. The magnitude of change is considered to be low as the changes for health outcomes relate to minor positive effects on mental health related morbidity and quality of life. Consequently, the significance of effect is determined to be minor positive.
Spatial Characteristics of the Transport Network and Usage (HD5)
- The proposed scheme would improve travel time and journey reliability on the A9, which could allow some individuals more time for health promoting pursuits, such as physical activity and recreation or self-care e.g. cooking healthy meals or resting. Improved separation between WCH and other road users helps to support safer and more convenient active travel modes which could encourage uptake of active travel, increasing physical activity levels with associated benefits to physical and mental health. Children traveling to and from school or afterschool activities would particularly benefit from the separation and improved safety for pathways along the A9. People using the train station would benefit from improved access with the Dunkeld & Birnam Station Pedestrian Underpass providing connection from the replacement car park at the top of Station Road to Platform 1 and Platform 2 of Dunkeld & Birnam Station. The underpass structure would include stairs and lifts and be fully accessible for walkers, wheelers and cyclists. This would increase accessibility for more vulnerable groups and reduce inequalities through providing better access to the public transport network.
- The sensitivity of the general population is low, however, the vulnerable group population, which may include people who are dependent on cars, such as people who are disabled, as well as children and parents going to school, is high. This high sensitivity reflects the importance of the A9 in accessing facilities in the wider area, and the importance of WCH provision for those who cannot use a car, such as children and some people with disabilities. The improvements to WCH infrastructure and railway station accessibility are likely to affect a large minority of the population in the long term with associated improvements to quality of life and health. The significance of effect is judged to be minor positive for the general population and Moderate positive for children, people with disabilities and WCH groups. This is on the basis that regular physical activity and improved access have a clear relationship with improved health and wellbeing.
Air Quality (HD6)
- Chapter 8 (Air Quality) has modelled the magnitude of change at sensitive human health receptors between the base year (2023) and proposed year of opening (2036). The modelling shows that levels would stay well below (<75%) the respective Air Quality Objectives (AQO) for NO2, PM10 or PM5 predicted at all of the human health receptors. While well below the AQOs, there would be some small increases (and at one modelled receptor a medium scale increase) in concentrations of air pollution (refer to Table 8.12 in Chapter 8 (Air Quality) for information on which pollutants and receptors). The medium level of increase would be at the Craigvinean Surgery. The GP surgery is frequented by vulnerable groups who are considered highly sensitive. However, the levels of NO2 modelled at this location were still well below the AQO requirements and also fall below the much more conservative NO2 and PM10 guideline levels recommended by WHO (2021). The levels are also very close to meeting the 5.0µg/m3 guideline for PM2.5 (5.5µg/m3 with the proposed scheme for 2036), so these changes are not considered significant.
- The sensitivity of the general population is low with overall good general health. However, the vulnerable group population, which may include people in very poor health or those with respiratory conditions who may be more susceptible to changes in air quality, have been assigned a high sensitivity. In population health terms the changes in air quality are judged to be negative, as more of the most impacted receptors would experience an increase in pollutant concentrations than a decrease. However, in terms of the overall population in the local community study area, the level of exposure to these changes would be very low, as the majority of the population would not be exposed to changes in air pollutant concentrations. Therefore, the magnitude of health change is judged to be low. This is not considered significant for either the general population or vulnerable groups as changes due to the proposed scheme would be well within the AQOs and the change in health baseline is likely to be slight based on the scale of change in air pollution concentrations. Therefore, the potential significance of effect is determined to be minor negative.
Noise and the Ambient Noise Environment (HD7)
- Chapter 15 (Noise and Vibration) has predicted the daytime and night-time noise levels at sample noise sensitive receptors in the opening year with and without the proposed scheme, and in the future assessment year with and without the proposed scheme (see Table 15.21 and Table 15.22). Reference to Chapter 15 (Noise and Vibration) should be made for further detail of these impacts with regards to the Significant Observed Adverse Effect Level (SOAEL) used as a metric in the noise and vibration assessment.
- During the daytime, the results show that in the short term, the majority (6 out of 9) of sample receptors would experience negligible to major beneficial changes (reductions in noise). Two receptors would experience negligible negative changes (increase in noise) and one receptor (Rowan Cottage) would experience a moderate negative change in noise in the short term (i.e. year 2036), a change of 3.1dB, which would be only just perceptible to the majority of people. In the long term (i.e. for the 2051 modelled year), the majority (5 out of 9) of sample receptors would experience negligible to minor beneficial changes (reductions in noise). Three receptors would experience negligible negative changes (increase in noise) and one receptor (Rowan Cottage) would experience a minor negative change in noise in the long term (i.e. year 2051), a change of 3.8dB, which would be only just perceptible to the majority of people.
- During the nighttime, the results show that in the short term, the majority (6 out of 9) of sample receptors would experience negligible to moderate beneficial changes (reductions in noise). Two receptors would experience negligible negative changes (increase in noise) and one receptor (Rowan Cottage) would experience a minor negative change in noise in the short term (i.e. year 2036), a change of 2.8dB. In the long term (i.e. for the 2051 modelled year), the majority (5 out of 9) of sample receptors would experience negligible to minor beneficial changes (reductions in noise). Three receptors would experience negligible negative changes (increase in noise) and one receptor (Rowan Cottage) would experience a minor negative change in noise in the long term (i.e. year 2051), a change of 3.4dB.
- In terms of population health, the changes to the noise environment predicted for the proposed scheme are judged to relate to a low magnitude of impact, with a small minority of the population expected to experience any noticeable change in the noise environment. This is likely to result in potential health outcomes such as a minor change in quality of life for most (i.e. long term annoyance from traffic noise), but for those exposed to the higher amount of traffic noise, there is potential for a minor change in morbidity (long term sleep disturbance and cardiovascular risk). The sensitivity of the general population is low with overall good general health. However, the vulnerable group population, which may include people with ASD (autism spectrum disorder) and those who suffer from anxiety who may be more susceptible to changes in noise and vibration, have been assigned a medium sensitivity on the basis that they will be habituated to traffic noise in the study area due to the baseline ambient noise conditions. Consequently, the significance of effect is determined to be minor negative for both the general population and the vulnerable groups.
Sources and Pathways of Potential Pollution (HD8)
- Chapter 13 (Geology and Soils) provides an assessment of risks from pollution and contaminated materials in soils and groundwater and potential pathways to human health receptors (i.e. people). There are potentially four active private water supplies that supply Murthly Castle and some residential properties. None of these have been identified as being in close proximity to the proposed scheme and are not at risk of water quality impairment due to accidental spillage. Therefore, there is limited likelihood of human health exposure to potential pollutants entering groundwater for the population. Table 13.19 of Chapter 13 (Geology and Soils) shows potential impacts on human health receptors from indirect pollutant pathways of windblown soil dust and fibres with a minor negative magnitude of impact on residential, open space and commercial human health receptors during operation (negligible for road users). Chapter 13 also identifies a Moderate significance of effect on residential receptors (the most sensitive receptors due to duration of potential exposure) and slight significance for open space and commercial/industrial receptors (high and medium sensitivity respectively). The assessment presented in Chapter 13 (Geology and Soils) is based on significance for individual receptors, whereas this assessment considers the impacts on population health.
- The health sensitivity of the general population is low and the likelihood of exposure for the general population is judged to be very low due to distance from potential contaminative sources of pollution and the potential for any occasional events being dependent on weather conditions. This indicates a minor negative potential significance of effect for the general population, as there is a suggestive relationship between changes resulting from the proposed scheme and health outcomes when considered in the context of baseline exposure to various contaminants over lifetimes of individuals within the population. Vulnerable groups are considered to be those residents in close proximity of the proposed scheme who are more likely to be frequently exposed to pollution pathways from the proposed scheme. Therefore, vulnerable groups are expected to have medium magnitude of unmitigated impact, resulting in a Moderate negative significance of effect.
Safety Associated with the Affected Road Network (HD9)
- A key objective of the proposed scheme is to reduce accident severity (see Chapter 2 (Need for the Scheme), Section 2.4). The inclusion of appropriately sized lay-bys would improve safety by providing drivers the opportunity to stop for a short time and rest or for drivers to leave the trunk road in the event of an emergency or breakdown. Grade separated junctions would improve safety through mitigating the need for potentially dangerous right turns across the path of traffic travelling in the opposite direction. Upgrading the road from single carriageway to dual carriageway could reduce the occurrence of driver frustration and would provide opportunity for safer overtaking. The provision of new grade separated crossing points of the A9 for WCH, such as the Murthy Underbridge and Birnam Junction Underbridge would improve safety for pedestrians and cyclists. The people who would benefit would include vehicle travellers of the A9 and WCH primarily using routes for recreational purposes.
- On account of the vulnerability of WCH to road collisions, the sensitivity of the population is judged to be high overall. The magnitude of these road safety improvements is judged to be medium. While the improvements relate to mortality or changes in morbidity (fatalities and severe injuries and trauma from road traffic collisions) the changes are deemed to affect a small minority of the population in the long-term. The significance of effect on population health is judged to be Moderate positive as the safety improvements are likely to affect a small change in health baseline and there is a clear relationship between road safety improvements and improved health outcomes.
Flood Risk (HD10)
- The FRA (Appendix A19.2) outlines some of the embedded mitigation design features of the proposed scheme to address flood risk , such as reducing extent of the proposed scheme located within the floodplain. The proposed scheme has been shown to have both beneficial and negative flood risk impacts.
- The proposed scheme mainline has been raised above the design flood event and, as a result, would largely remain safe and operational during times of flood. Unmitigated, the proposed scheme would increase the risk of flooding associated with principal watercourses to flood sensitive receptors, including residential properties in the Braan floodplain. However, provision of indirect flood storage, in combination with additional mitigation measures, has resulted in very limited and small localised areas of minor adverse impacts close to the river bank. These are minor changes in flood depth and extent; largely within the CPO for the proposed scheme or in areas of riparian woodland. It has been demonstrated that there are no residual adverse impacts to sensitive receptors.
- The FRA also assesses that there would be both beneficial impacts and adverse impacts associated with minor watercourses. Beneficial impacts of flood risk are noted for parts of the A9, A923, residential and commercial properties in Little Dunkeld, Perth Road, Highland Main Line railway and woodland. Slight adverse impacts of significance of flood risk are noted for parts of the A9 and woodland. The FRA assesses impacts on surface flood risk and groundwater flood risk as negligible.
- On this basis, for the general population the proposed scheme is expected to be beneficial for health in reducing flood risk. However, for those residents in the Braan floodplain, the health effect is negative, both as a result of actual risk and a likelihood of increased anxiety. Such events would be occasional and affect a small minority of the population but would be a long-term risk, meaning the health magnitude is assessed as medium for the vulnerable groups. Consequently, the significance of effect is determined to be minor positive for the general population and Moderate negative for vulnerable groups.
Summary of Potential Operational Impacts
- Table 18.14 provides a summary of the potential impacts on health determinants and likely significance of effect for health outcomes during operation prior to any additional mitigation.
Table 18.14: Operation Summary – Potential Effects on Health and Wellbeing Determinants and Likely Health Outcomes
|
Health Determinants |
Sensitivity |
Potential Magnitude |
Potential Significance |
|
HD1: community, recreational and education facilities and severance/separation of communities from such facilities |
Low (general population) High (vulnerable groups) |
Low Low |
Minor positive Minor positive |
|
HD2: landscape amenity and green/open space and severance/separation of communities from such facilities |
Low (general population and vulnerable groups) |
Low |
Minor negative |
|
HD3: healthcare facilities and severance/separation of communities from such facilities |
Low (general population) High (vulnerable groups) |
Low Low |
Minor positive Moderate positive |
|
HD4: community identity, culture, resilience and influence |
Low (general population) High (vulnerable groups) |
Low Low |
Minor positive Minor positive |
|
HD5: spatial characteristics of the transport network and usage in the area |
Low (general population) High (vulnerable groups) |
Medium Medium |
Minor positive Moderate positive |
|
HD6: air quality |
Low (general population) High (vulnerable groups) |
Low Low |
Minor negative Minor negative |
|
HD7: noise and the ambient noise environment |
Low (general population) Medium (vulnerable groups) |
Low Low |
Minor negative Minor negative |
|
HD8: sources and pathways of potential pollution |
Low (general population) Medium (vulnerable groups) |
Low Medium |
Minor negative Moderate negative |
|
HD9: safety associated with the existing affected road network |
High (vulnerability of WCH to road traffic collisions) |
Medium |
Moderate positive |
|
HD10: flood risk |
Low (general population) Medium (vulnerable groups) |
Low Medium |
Minor positive Moderate negative |
Mitigation
- The most important mitigation for effects on social wellbeing during construction is likely to be effective communication and engagement, which will help address people’s individual concerns and also help them plan their daily lives around possible times of disruption. This mitigation will be delivered through standard mitigation commitment SMC-S3 which requires the Contractor to appoint a Community Liaison Officer to help keep the community informed and to be a point of contact throughout the construction period. This will help mitigate construction impacts relating to health determinant HD4 (Community identity, culture, resilience and influence) as it will enable people to better understand the proposals, arrange their daily lives around the works and be able to raise specific concerns so that the Contractor can take reasonable steps to reduce community effects.
- Chapter 16 (Population - Land use) and Chapter 17 (Population - Accessibility) set out mitigation measures which are relevant for reducing potential health effects relating to health determinants HD1 (community, recreational and education facilities), HD2 (landscape amenity and green/open space) and HD3 (healthcare facilities) as they include mitigation for impacts on accessibility and land use. Mitigation commitment SMC-LU1 and SMC-LU2 would mitigate potential impacts on access to the Dunkeld & Birnam Recreation Club (see Community, Recreational and Education Facilities (HD1) in Section 18.4) and the Craigvinean Surgery (see Healthcare Facilities (HD3) in Section 18.4) as the implementation of these commitments would ensure access is maintained. Mitigation commitment SMC-AT4 requires the Contractor to produce a traffic management plan with measures to avoid or reduce disruption to road traffic. This would also help mitigate effects on access to healthcare facilities described under HD3 in paragraphs 18.4.6 – 18.4.8.
- Chapter 17 (Population - Accessibility) sets out mitigation for accessibility. Standard mitigation commitments SMC-AT1 – SMC-AT8 and P02-AT1 – P02-AT15 would reduce the effects on the transport network and usage (as described under Spatial Characteristics of the Transport Network and Usage (HD5) in Section 18.4) and on road safety (as described under Safety Associated with the Affected Road Network (HD9) in Section 18.4). Standard and specific mitigation commitments during construction set out requirements for WCH route diversions, safety and signage, and require the Contractor to prepare a traffic management plan that will include measures to avoid or reduce disruption to the road traffic in accordance with relevant guidance, and expectations for accessibility provision and surfacing for new or maintained WCH routes. To reduce disruption for those using the railway network and allow people to find alternative transport routes, advance notice will be given of disruption to rail services as a result of the temporary closure of Dunkeld & Birnam Station during construction of the underpass.
- Chapter 10 (Landscape) and Chapter 11 (Visual) set out mitigation measures which are relevant for reducing potential health effects relating to health determinant HD2 (landscape amenity and green/open space). This includes appropriate lighting designs to mitigate light pollution.
- Chapter 8 (Air Quality), Chapter 13 (Geology and Soils), Chapter 15 (Noise and Vibration) and Chapter 19 (Road Drainage and the Water Environment) set out mitigation measures which are relevant to controlling pollution and are therefore relevant to reducing health effects relating to health determinants HD6 (air quality), HD7 (noise and ambient noise environment) and HD8 (sources and pathways of pollution).
- Chapter 19 (Road Drainage and the Water Environment) also sets out mitigation for flood risk relevant to health determinant HD10 (flood risk).
- No specific further mitigation measures for human health have been identified as it is expected that the mitigation requirements identified as standard, or by other topics of the EIA, provide for human health protection.
- The proposed scheme assessed within this chapter is the result of an iterative design process which had incorporated beneficial elements into the design throughout the process. For example, improved and safer access for road users and WCH, and improved access and reduced severance for Dunkeld & Birnam Station through the provision of a fully accessible underpass to both Platforms 1 and 2. As a result, no specific enhancement measures have been identified for human health. However, there are enhancement measures included in Chapter 22 (Schedule of Environmental Commitments) that are considered relevant for human health and would help the scheme achieve the Community Objectives (as set out in Table 18.2). These enhancement measures include:
- P02-CH06 and P02-CH09: Interpretation boards presenting interpretive information will be installed at suitable publicly accessible locations to enhance people’s understanding of, and their engagement with Murphy Castle and Dunkeld & Birnam Station. This would help to preserve and enhance the integrity of the unique and rich historical and cultural features of the Dunkeld, Birnam and Inver communities, thereby supporting wellbeing and the local economy (as per Community Objective 7).
- P02-LV9, P02-LV21, P02-LV24 and PO2-LV26: The design of Sustainable Drainage Solutions Features (Ponds, Wetlands, Basins, Swales and Geo-Cellular Storage Areas) (P02-LV9), the proposed planting relating to road users P02-LV21), design of the new B867 bridge to form a welcoming and dramatic ‘gateway’ to Birnam (P02-LV24), and Dunkeld Junction Gateway to the Highlands Feature Landscape (P02-LV26) will be refined to not only mitigate visual impact but enhance visual amenity. This would help to protect and enhance the scenic beauty and natural heritage of the area and its distinctive character and quality (as per Community Objective 2).
- P02-LV25: The design of the pedestrian underpass will be well-lit and include a series of large integrated interpretive/artistic elements to enhance the experience of walking through the underpass. This would help to encourage use of the underpass and improve access to the train station.
Residual Effects
- The residual effects are those that remain following the implementation of the proposed mitigation measures outlined in Section 18.5 and other relevant chapters. Table 18.15 provides a summary of the mitigation measures proposed that are relevant to each health determinant and the residual effects that are anticipated.
Table 18.15: Significance of Residual Effects
|
ID |
Health Determinant |
Mitigation Measures |
Description of Residual Effect |
Residual Significance |
|
Construction |
||||
|
HD1 |
Community, recreational and education facilities |
SMC-LU1 SMC-LU2 |
Implementation of standard mitigation would reduce potential health effects on high sensitivity groups to negligible through ensuring continued access to community facilities. |
Negligible negative (general population and vulnerable groups) |
|
HD2 |
Landscape amenity and green/open space |
SMC-LV1 SMC-LV2 SMC-LV3 SMC-LV4 SMC-LV5 SMC-LV6 SMC-LV7 SMC-LU1 SMC-LU2 SMC-AT1 SMC-AT2 |
Implementation of standard mitigation would reduce impacts on access to green/open space (i.e. community land or public rights of way to the countryside) as well as reduce impacts on landscape amenity. The residual magnitude after mitigation is expected to remain as low on the basis that a loss of tranquillity and visual amenity would still occur during the construction phase. |
Minor negative (general population and vulnerable groups) |
|
HD3 |
Healthcare facilities |
SMC-LU1 SMC-LU2 SMC-AT4 SMC-AT5 SMC-AT6 |
Implementation of standard mitigation would ensure continued access to local healthcare facilities within the Birnam and Dunkeld Communities as well as to hospitals and healthcare services normally access via the A9. While the magnitude of impact on access is expected to remain as low, the provision of advance information as required in the traffic management plan is expected to inform people to the extent that they can appropriately plan their journeys to healthcare appointments, reducing the significance of effect on highly sensitive groups. |
Minor negative (general population and vulnerable groups) |
|
HD4 |
Community identity, culture, resilience and influence |
SMC-S3 SMC-LU3 SMC-LU4 |
The implementation of standard mitigation in the form of the appointment of a Community Liaison Officer, a liaison team and dedicated helpline, will help ensure that the community is kept informed of the works and have channels through which they can make enquiries and voice concerns relating to the construction phase. Additionally, consultation with landowners will be used to reduce disturbance as far as practicable and notice will be given of intention to commence works. This would help people plan their lives around the works, and have a degree of influence, which is likely to reduce the residual significance for sensitive groups. |
Minor negative (general population and vulnerable groups) |
|
HD5 |
Spatial characteristics of the transport network and usage |
SMC-AT1 to AT8 P02-AT9 to AT15 |
Standard and project-specific mitigation would limit disruption to roads, public transport and routes for WCH during the construction phase as far as practicable. Vulnerable groups would have higher sensitivity to any form of disruption or diversion and more limited capacity to adapt, however implementation of the mitigation coupled with the temporary nature of the construction stage is judged to have a marginal impact on health inequalities or change in health status of these population groups. |
Minor negative (general population and vulnerable groups) |
|
HD6 |
Air quality |
SMC-AQ1 SMC-AQ2 P02-AQ1 to P02AQ11 |
Standard and project-specific mitigation for air quality would limit human exposure to dust and construction air pollution and would provide information to local communities. The residual magnitude of health impact is expected to remain as low due to the links between air pollution and health, but any change in population health is not expected to be significant. |
Negligible negative (general population) Minor negative (vulnerable groups) |
|
HD7 |
Noise and the ambient noise environment |
SMC-S3 SMC-NV1 to NV2 |
Effective communication via the Community Liaison Officer, implementation of a Noise and Vibration Management Plan and use of Best Practicable Means to limit noise, will mitigate effects of construction noise to a degree, including a likelihood of reducing community concerns. Nevertheless, there is still a likelihood of a moderate change in quality of life due to occasional sleep disturbance (especially for shift workers) and annoyance, which is judged to be a low magnitude of health impact. Effects are likely to remain significant for highly sensitive groups. |
Minor negative (general population) Moderate negative (vulnerable groups) |
|
HD8 |
Sources and pathways of potential pollution |
SMC-S3 SMC-LU9 SMC-M2 SMC-G1 to SMC-G9 and SMC-G12 to G14 SMC-W3 SMC-W6 to SWC-W12 |
Standard mitigation will ensure appropriate investigation of areas of potential contamination, classification of materials, handling, storage, re-use or disposal of materials as appropriate, to avoid significant risks of significant harm to health. The residual magnitude of impact during construction on population health is judged to be low as exposure to substances from the site would be reduced to occasional events in the short-term. With effective communication, concerns are likely to be alleviated such that health concerns are not significant. |
Minor negative (general population and vulnerable groups) |
|
HD9 |
Safety associated with the affected road network |
SMC-AT2 to AT7 |
Standard mitigation for traffic management and to ensure safe crossings and diversions for WCH routes would reduce safety risks such that the likelihood of a collision during construction is very low. The residual magnitude is judged to be low. However, due to the sensitivity of communities to road safety issues, the residual significance is judged to remain significant for vulnerable groups. |
Minor negative (general population) Moderate negative (vulnerable groups) |
|
HD10 |
Flood risk |
SMC-S1 SMC-W2 |
Mitigation would not change the significance of effect for human health, therefore, the residual effects are as described in Section 18.4 and summarised in Table 18.13. |
Minor negative (general population and vulnerable groups) |
|
Operation |
||||
|
HD1 |
Community, recreational and education facilities |
N/A |
Mitigation is not required, therefore, the significance of effect for human health is as described in Section 18.4 and summarised in Table 18.14. |
Minor positive (general population and vulnerable groups) |
|
HD2 |
Landscape amenity and green/open space |
P02-LV8 to P02-LV27 |
Mitigation would not change the significance of effect for human health, therefore, the residual effects are as described in Section 18.4 and summarised in Table 18.14. |
Minor negative (general population and vulnerable groups) |
|
HD3 |
Healthcare facilities |
N/A |
Mitigation is not required, therefore, the significance of effect for human health is as described in Section 18.4 and summarised in Table 18.14. |
Minor positive (general population) Moderate positive (vulnerable groups) |
|
HD4 |
Community identity, culture, resilience and influence |
N/A |
Mitigation is not required, therefore, the significance of effect for human health is as described in Section 18.4 and summarised in Table 18.14. |
Minor positive (general population and vulnerable groups) |
|
HD5 |
Spatial characteristics of the transport network and usage |
N/A |
Mitigation is not required, therefore, the significance of effect for human health is as described in Section 18.4 and summarised in Table 18.14. |
Minor positive (general population) Moderate positive (vulnerable groups) |
|
HD6 |
Air quality |
N/A |
The residual magnitude of health impact is expected to remain as low due to the links between air pollution and health, but any change in population health is not expected to be significant for the general population as well as vulnerable groups. |
Minor negative (general population and vulnerable groups) |
|
HD7 |
Noise and the ambient noise environment |
P02-NV03 |
Proposed installation of a noise barrier would reduce noise effects for residences in the vicinity of Rowan Cottage to a level of change less than 3dB which is unlikely to be perceptible compared to the do-nothing scenario in both the short and long term. With the mitigation in place and taking into account that very few people would be affected, the residual magnitude of change on health is judged to be negligible compared to the do-nothing scenario. |
Negligible (general population) Minor negative (vulnerable groups) |
|
HD8 |
Sources and pathways of potential pollution |
SMC-S3 SMC-M2 SMC-G1 to SMC-G9 and SMC-G12 to G14 |
Standard mitigation will reduce the risk of exposure pathways between a potential pollution source and human population to avoid significant risks of significant harm to health. The residual magnitude of impact during operation on population health is judged to be negligible. |
Negligible (general population and vulnerable groups) |
|
HD9 |
Safety associated with the affected road network |
N/A |
Mitigation is not required, therefore, the significance of effect for human health is as described in Section 18.4 and summarised in Table 18.14. |
Moderate positive (general population and vulnerable groups) |
|
HD10 |
Flood risk |
SMC-W15 |
Following the implementation of mitigation, including compensatory flood storage, culverts and monitoring programmes (see Appendix 19.2: Flood Risk Assessment), the residual flood risk is neutral. The residual magnitude of impact during operation on population health is judged to be low for concerned vulnerable groups, primarily as a result of increased anxiety affecting a minority of the population. |
Minor positive (general population) Minor negative (vulnerable groups) |
Compliance Against Plans and Policy
- DMRB LA 104 states that environmental assessment, reporting and monitoring shall meet the requirements of the national planning policy for each relevant Overseeing Organisation.
- Appendix A3.1 (Assessment of Policy Compliance) provides a review of national and local policy documents which are of relevance to the assessment undertaken and reported in this chapter in accordance with DMRB guidance. The compliance assessment undertaken in Appendix A3.1 focuses principally on the long-term effects of the proposed scheme, rather than the short term, temporary effects from construction.
- National policy objectives of relevance to this assessment are provided in the National Planning Framework 4 (Scottish Government, 2023a). The Perth & Kinross Local Development Plan 2 (Perth & Kinross Council, 2019) is also of relevance.
Summary of Policy Compliance
- Overall, the design and assessment of the proposed scheme has had regard to, and is compliant with, policy objectives to reduce effects on human health. A full assessment can be found in Table A3.1-11 of Appendix A3.1 (Assessment of Policy Compliance).
Statement of Significance
- During construction, there is a likelihood of negative effects of Moderate significance on health and wellbeing of vulnerable groups related to construction noise (HD7 – noise and the ambient noise environment). Additionally, during construction there is a likelihood of negative effects of Moderate significance on health and wellbeing of vulnerable groups related to safety risks (HD9 – safety associated with the affected road network). However, these effects would be short-term and reversible on completion of the works.
- During operation, there is a likelihood of positive effects of Moderate significance on health and wellbeing of vulnerable groups in relation to healthcare facilities (HD3 - healthcare facilities) and in transport-related health determinant HD5 - spatial characteristics of the transport network and usage. There is a likelihood of positive effects of Moderate significance on health and wellbeing for the general population and vulnerable groups related to transport (HD9 – safety associated with the road network).
- It is expected that the health and wellbeing of vulnerable groups will benefit from the improvements to the road design incorporated in the proposed scheme, such as improved access to healthcare services, improved road safety and improvements in local connectivity for walkers and wheelers.
References
American Hospital Association (2020). Social Determinants of Health Series: Promoting Healthy Behaviors. (Accessed February 2025).
Anciaes, P.R., Boniface, S., Dhanani, A., Mindell, J.S. and Groce, N. (2016). Urban transport and community severance: Linking research and policy to link people and places. (Accessed February 2025).
Anciaes, P.R., Metcalfe, P.J. and Heywood, C. (2017). Social impacts of road traffic: Perceptions and priorities of local residents. Impact assessment and project appraisal. (Accessed February 2025).
Bassett D., Pucher J., Buehler R., Thompson D. and Crouter S. (2008). Walking, cycling, and obesity rates in Europe, North America and Australia. (Accessed February 2025).
Bray, I., Reece, R., Sinnett, D., Martin, F. and Hayward, R. (2022). Exploring the role of exposure to green and blue spaces in preventing anxiety and depression among young people aged 14–24 years living in urban settings: A systematic review and conceptual framework. (Accessed February 2025).
British Medical Association (2012). Healthy transport = Healthy lives. (Accessed February 2025).
Caldwell L.L. (2005). Leisure and health: Why is leisure therapeutic? (Accessed February 2025).
Chen, J. and Hoek, G. (2020). Long-term exposure to PM and all-cause and cause-specific mortality: A systematic review and meta-analysis. (Accessed February 2025).
Clark, C., Crumpler, C. and Notley, H. (2020). Evidence for environmental noise effects on health for the United Kingdom policy context: a systematic review of the effects of environmental noise on mental health, wellbeing, quality of life, cancer, dementia, birth, reproductive outcomes, and cognition. (Accessed February 2025).
Cooke, A., Friedli, L., Coggins, T., Edmonds, N., Michaelson, J., O’Hara, K., Snowden, L., Stansfield, J., Steuer, N. and Scott-Samuel, A. (2011). Mental Wellbeing Impact Assessment. (Accessed February 2025).
Coventry, P.A., Brown, J.V.E., Pervin, J., Brabyn, S., Pateman, R., Breedvelt, J., Gilbody, S., Stancliffe, R., McEachan, R. and White, P.C.L. (2021). Nature-based outdoor activities for mental and physical health: Systematic review and meta-analysis. (Accessed February 2025).
Dunkeld & Birnam Tourist Association (no date). Meet the Locals. Available at: https://www.dunkeldandbirnam.org.uk/meet-the-locals (Accessed November 2024).
Fancourt D. and Finn S. (2019) What is the evidence on the role of the arts in improving health and well-being? A scoping review. (Accessed February 2025).
Gascon, M., Triguero-Mas, M., Martínez, D., Dadvand P., Forns, J., Plasència, A. and Nieuwenhuijsen, M.J. (2015). Mental health benefits of long-term exposure to residential green and blue spaces: a systematic review. (Accessed February 2025).
Holt-Lunstad J., Smith T.B. and Layton J.B. (2010). Social relationships and mortality risk: a meta-analytic review. (Accessed February 2025).
Houlden, V., Weich, S., Porto de Albuquerque, J., Jarvis, S. and Rees, K. (2018). The relationship between greenspace and the mental wellbeing of adults: A systematic review. (Accessed February 2025).
International Association of Impact Assessment (2020). Human health: Ensuring a high level of protection. (Accessed February 2025).
Kovacevic, J., Miskulin, M., Degnecic, D., Vcev, A., Leovic, D., Sislijagic, S., Simic, I., Palenkic, H., Vcev, I. and Miskulin, I. (2020). Predictors of Mental Health Outcomes in Road Traffic Accident Survivors. (Accessed February 2025).
Leigh-Hunt, N., Bagguley, D., Bash, K., Turner, V., Turnbull, S., Valtorta, N. and Caan, W. (2017). An overview of systematic reviews on the public health consequences of social isolation and loneliness. (Accessed February 2025).
Lyon R.M., Cobbe S.M., Bradley J.M. and Grubb N.R. (2004). Surviving out of hospital cardiac arrest at home: a postcode lottery? (Accessed February 2025).
Marmot, M., Allen, J., Boyce, T., Goldblatt, P. and Morrison J. (2020). Health Equity in England: The Marmot Review 10 Years On. (Accessed February 2025).
Mindell, J.S. and Karlsen, S. (2012). Community severance and health: what do we actually know? (Accessed February 2025).
National Highways, Transport Scotland, Welsh Government, Department for Infrastructure Northern Ireland (2019). Standards for Highways Design Manual for Roads and Bridges. LA 104 - Environmental assessment and monitoring. (Accessed February 2025).
National Highways, Transport Scotland, Welsh Government, Department for Infrastructure Northern Ireland (2020). Standards for Highways Design Manual for Roads and Bridges. LA 112 - Population and human health. (Accessed February 2025).
National Highways, Transport Scotland, Welsh Government, Department for Infrastructure Northern Ireland (2024). Standards for Highways Design Manual for Roads and Bridges. LA 105 - Air quality. (Accessed February 2025).
National Records of Scotland (2023). List of Data Tables. Section 6: Deaths – Causes (Table 6.03). (Accessed October 2024).
Orellano, P., Reynoso, J., Quaranta, N., Bardach, A. and Ciapponi, A. (2020). Short-term exposure to particulate matter (PM10 and PM2.5), nitrogen dioxide (NO2), and ozone (O3) and all-cause and cause-specific mortality: Systematic review and meta-analysis. (Accessed February 2025).
Perth & Kinross Council (2018). Mental Health and Wellbeing Action Plan. (Accessed February 2025).
Perth & Kinross Council (2019). Perth and Kinross Council Local Development Plan 2. (Accessed February 2025).
Public Health England (2020). Flooding and health: national study. (Accessed February 2025).
Public Health Scotland (2024a). ScotPHO Profiles Tool. (Accessed November 2024).
Public Health Scotland (2024b). Open space and the environment. (Accessed November 2024).
Pyper, R., Waples, H., Beard, C., Barratt, T., Hardy, K., Turton, P., Netherton, A., McDonald, J., Buroni, A., Bhatt, A., Phelan, E., Scott, I., Fisher, T., Christian, G., Ekermawi, R., Devine, K., McClenaghan, R., Fenech, B., Dunne, A., Hodgson, G., Purdy, J. and Cave, B. (2022a). IEMA Guide to Determining Significance for Human Health in Environmental Impact Assessment. (Accessed February 2025).
Pyper, R., Lamming, M., Beard C., Waples, H., Birley, M., Buroni, A., Douglas, M., Turton, P., Hardy, K., Netherton, A., McClenaghan, R., Barratt, T., Bhatt, A., Fenech, B., Dunne, A., Hodgson, G., Gibson, G., Purdy, J. and Cave, B. (2022b). IEMA Guide to Effective Scoping of Human Health in Environmental Impact Assessment. (Accessed February 2025).
Rompel, S., Schneider, A., Peters, A., Kraus, U. and INGER Study Group (2021). Sex/gender-differences in the health effects of environmental noise exposure on hypertension and ischemic heart disease—a systematic review. (Accessed February 2025).
Royal College of Physicians (2016). Every breath we take: the lifelong impact of air pollution. (Accessed February 2025).
Scotland’s Census (2022a). Demography and migration: Table UV102b - Age (20) by sex - Intermediate Zone - Data Zone 2011 by Age by Sex by Individuals. Available at: https://www.scotlandscensus.gov.uk/search-the-census#/search-by (Accessed October 2024).
Scotland’s Census (2022b). Demography and migration: Table UV102b - Age (20) by sex - Council Area 2019 by Age by Sex by Individuals. (Accessed October 2024).
Scotland’s Census (2022c). Demography and migration: Table UV102b - Age (20) by sex - Country by Age by Sex by Individuals. (Accessed October 2024).
Scotland’s Census (2022d). Demography and migration: Table UV102b - Age by single year - Intermediate Zone - Data Zone 2011 by Age by Sex by Individuals. (Accessed October 2024).
Scotland’s Census (2022e). Demography and migration: Table UV102b - Age single year (by sex) - Country by Age by Sex by Individuals. (Accessed October 2024).
Scotland’s Census (2022f). Health, disability and unpaid care: Table UV302 - General health - Intermediate Zone - Data Zone 2011 by General Health. (Accessed October 2024).
Scotland’s Census (2022g). Health, disability and unpaid care: Table UV302 - General health - Council Area 2019 by General Health. (Accessed October 2024).
Scotland’s Census (2022h). Health, disability and unpaid care: Table UV302 - General health - Country by General Health. (Accessed October 2024).
Scotland’s Census (2022i). Health, disability and unpaid care: Table UV303b - Disability by age (6) - Intermediate Zone - Data Zone 2011 by Age by Disability. (Accessed October 2024).
Scotland’s Census (2022j). Health, disability and unpaid care: Table UV303b - Disability by age (6) - Council Area 2019 by Age by Disability. (Accessed October 2024).
Scotland’s Census (2022k). Health, disability and unpaid care: Table UV303b - Disability by age (6) - Country by Age by Disability. (Accessed October 2024).
Scottish Environment Protection Agency (2017). Regulatory Method (WAT-RM-11) Licensing Groundwater Abstractions including Dewatering. V6. (Accessed February 2025).
Scottish Government (2017). Mental Health Strategy 2017 – 2027. (Accessed February 2025).
Scottish Government (2018). Public Health Priorities for Scotland. (Accessed February 2025).
Scottish Government (2019). National Performance Framework. (Accessed February 2025).
Scottish Government (2020a). Scottish Index of Multiple Deprivation 2020 Interactive Mapping. (Accessed October 2024).
Scottish Government (2020b). Scottish Index of Multiple Deprivation 2020v2 – indicators. (Accessed October 2024).
Scottish Government (2023a). National Planning Framework 4. Available at: https://www.gov.scot/publications/national-planning-framework-4/ (Accessed February 2025).
Scottish Government (2023b). Mental health and wellbeing strategy. Available at: https://www.gov.scot/publications/mental-health-wellbeing-strategy/ (Accessed February 2025).
Simonsen, S. A., Andresen, M., Michelsen, L., Viereck, S., Lippert, F. K., and Iversen, H. K. (2014). Evaluation of pre-hospital transport time of stroke patients to thrombolytic treatment. Available at: https://doi.org/10.1186/s13049-014-0065-z (Accessed February 2025).
Stanke, C., Murray, V., Amlôt, R., Nurse, J. and Williams, R. (2012). The effects of flooding on mental health: Outcomes and recommendations from a review of the literature. Available at: https://pubmed.ncbi.nlm.nih.gov/23066515/ Accessed February 2025).
Transport Scotland (2013). A9 Dualling Programme Strategic Environmental Assessment (SEA) Report. TSSEA/PASS01.
Transport Scotland (2020). National Transport Strategy 2. Available at: https://www.transport.gov.scot/publication/national-transport-strategy-2/ (Accessed February 2025).
Transport Scotland (2022). Strategic Transport Projects Review (STPR2). Available at: https://www.transport.gov.scot/our-approach/strategy/strategic-transport-projects-review-2/stpr2-strategic-approach/ (Accessed February 2025).
United Nations (2015.) Sustainable Development Goals. Available at: https://sdgs.un.org/goals (Accessed February 2025).
Wang, M., Li, H., Huang, S., Qian, Y., Steenland, K., Xie, Y., Papatheodorou, S. and Shi, L. (2021). Short-term exposure to nitrogen dioxide and mortality: A systematic review and meta-analysis. Available at: https://pubmed.ncbi.nlm.nih.gov/34331919/ (Accessed February 2025).
Winkler, M.S., Viliani, F., Knoblauch, A.M., Cave, B., Divall, M., Ramesh, G., Harris-Roxas, B. and Furu, P. (2021) Health Impact Assessment International Best Practice Principles. Special Publication Series No. 5. Available at: https://www.researchgate.net/publication/352573139_Health_impact_assessment_international_best_practice_principles_International_Association_for_Impact_Assessment (Accessed February 2025).
World Health Organization (1948). Constitution of the World Health Organization. Available at: https://www.who.int/about/governance/constitution (Accessed February 2025).
World Health Organization (2018). ENVIRONMENTAL NOISE GUIDELINES for the European Region. Available at: https://iris.who.int/bitstream/handle/10665/279952/9789289053563-eng.pdf?sequence=1 (Accessed February 2025).
World Health Organization (2020). Ten Chemicals of public health concern. Available at: https://www.who.int/news-room/photo-story/photo-story-detail/10-chemicals-of-public-health-concern (Accessed February 2025).
World Health Organization (2021). WHO global air quality guidelines: particulate matter (PM2.5 and PM10), ozone, nitrogen dioxide, sulfur dioxide and carbon monoxide. Available at: https://www.who.int/publications/i/item/9789240034228 (Accessed February 2025).
World Health Organization (2023a). Assessing the value of urban green and blue spaces for health and well-being. Available at: https://www.who.int/europe/publications/i/item/WHO-EURO-2023-7508-47275-69347 (Accessed November 2024).
World Health Organization (2023b). Global status report on road safety 2023. Available at: https://iris.who.int/bitstream/handle/10665/375016/9789240086517-eng.pdf?sequence=1 (Accessed February 2025).
World Health Organization (2024). Compendium of WHO and other UN guidance on health and environment. Available at: https://reliefweb.intworld/compendium-who-and-other-un-guidance-health-and-environment-2024-update (Accessed February 2025).
World Health Organization (no date). Road traffic mortality. Available at: https://www.who.int/data/gho/data/themes/topics/topic-details/GHO/road-traffic-mortality#:~:text=Road%20traffic%20injuries%20are%20currently,safety%20in%20a%20holistic%20manner (Accessed February 2025).